

Mild hypoglycemia is independently associated with increased mortality in the critically ill
- PMID: 21787410
- PMCID: PMC3387616
- DOI: 10.1186/cc10322
Mild hypoglycemia is independently associated with increased mortality in the critically ill
Abstract
Introduction: Severe hypoglycemia (blood glucose concentration (BG) < 40 mg/dL) is independently associated with an increased risk of mortality in critically ill patients. The association of milder hypoglycemia (BG < 70 mg/dL) with mortality is less clear.
Methods: Prospectively collected data from two observational cohorts in the USA and in The Netherlands, and from the prospective GLUCONTROL trial were analyzed. Hospital mortality was the primary endpoint.
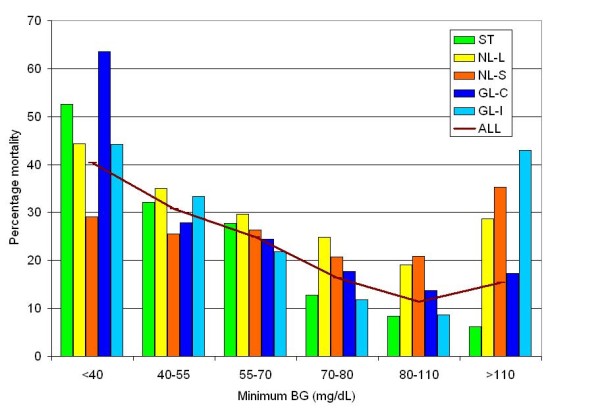
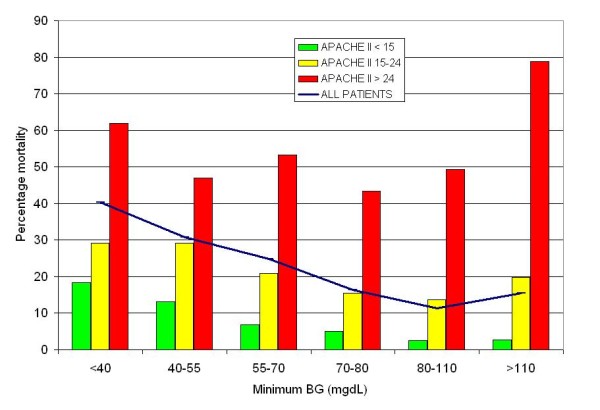
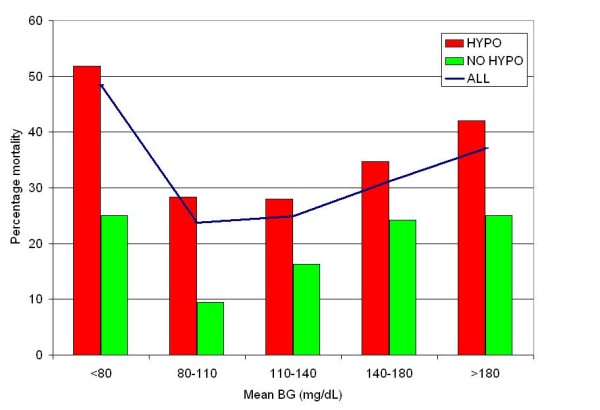
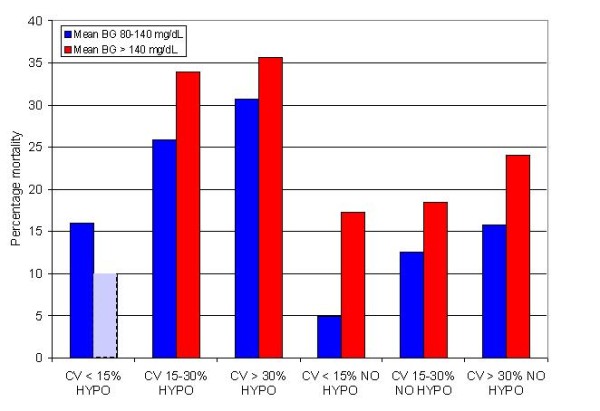
Results: We analyzed data from 6,240 patients: 3,263 admitted to Stamford Hospital (ST), 2,063 admitted to three institutions in The Netherlands (NL) and 914 who participated in the GLUCONTROL trial (GL). The percentage of patients with hypoglycemia varied from 18% to 65% among the different cohorts. Patients with hypoglycemia experienced higher mortality than did those without hypoglycemia even after stratification by severity of illness, diagnostic category, diabetic status, mean BG during intensive care unit (ICU) admission and coefficient of variation (CV) as a reflection of glycemic variability. The relative risk (RR, 95% confidence interval) of mortality associated with minimum BG < 40, 40 to 54 and 55 to 69 mg/dL compared to patients with minimum BG 80 to 109 mg/dL was 3.55 (3.02 to 4.17), 2.70 (2.31 to 3.14) and 2.18 (1.87 to 2.53), respectively (all P < 0.0001). The RR of mortality associated with any hypoglycemia < 70 mg/dL was 3.28 (2.78 to 3.87) (P < 0.0001), 1.30 (1.12 to 1.50) (P = 0.0005) and 2.11 (1.62 to 2.74) (P < 0.0001) for the ST, NL and GL cohorts, respectively. Multivariate regression analysis demonstrated that minimum BG < 70 mg/dL, 40 to 69 mg/dL and < 40 mg/dL were independently associated with increased risk of mortality for the entire cohort of 6,240 patients (odds ratio (OR) (95% confidence interval (CI)) 1.78 (1.39 to 2.27) P < 0.0001), 1.29 (1.11 to 1.51) P = 0.0011 and 1.87 (1.46 to 2.40) P < 0.0001) respectively.
Conclusions: Mild hypoglycemia was associated with a significantly increased risk of mortality in an international cohort of critically ill patients. Efforts to reduce the occurrence of hypoglycemia in critically ill patients may reduce mortality.
Figures
Comment in
-
Hypoglycemia in critically ill adults--association yes, causation not proven.Crit Care. 2011;15(6):1012. doi: 10.1186/cc10427. Epub 2011 Nov 30. Crit Care. 2011. PMID: 22188732 Free PMC article.
Similar articles
-
Diabetic status and the relation of the three domains of glycemic control to mortality in critically ill patients: an international multicenter cohort study.Crit Care. 2013 Mar 1;17(2):R37. doi: 10.1186/cc12547. Crit Care. 2013. PMID: 23452622 Free PMC article.
-
Mild hypoglycemia is strongly associated with increased intensive care unit length of stay.Ann Intensive Care. 2011 Nov 24;1:49. doi: 10.1186/2110-5820-1-49. Ann Intensive Care. 2011. PMID: 22115519 Free PMC article.
-
Glucose Control, Diabetes Status, and Mortality in Critically Ill Patients: The Continuum From Intensive Care Unit Admission to Hospital Discharge.Mayo Clin Proc. 2017 Jul;92(7):1019-1029. doi: 10.1016/j.mayocp.2017.04.015. Epub 2017 Jun 20. Mayo Clin Proc. 2017. PMID: 28645517
-
Intensive insulin therapy and mortality among critically ill patients: a meta-analysis including NICE-SUGAR study data.CMAJ. 2009 Apr 14;180(8):821-7. doi: 10.1503/cmaj.090206. Epub 2009 Mar 24. CMAJ. 2009. PMID: 19318387 Free PMC article. Review.
-
The impact of premorbid diabetic status on the relationship between the three domains of glycemic control and mortality in critically ill patients.Curr Opin Clin Nutr Metab Care. 2012 Mar;15(2):151-60. doi: 10.1097/MCO.0b013e32834f0009. Curr Opin Clin Nutr Metab Care. 2012. PMID: 22234163 Review.
Cited by
-
Body mass index-mortality relationship in severe hypoglycemic patients with type 2 diabetes.Am J Med Sci. 2015 Mar;349(3):192-8. doi: 10.1097/MAJ.0000000000000382. Am J Med Sci. 2015. PMID: 25526505 Free PMC article.
-
Composite Metric of Glycemic Control Q-Score Is Elevated in Pediatric and Adolescent/Young Adult Hematopoietic Stem Cell Transplant Recipients.Diabetes Technol Ther. 2023 Feb;25(2):116-121. doi: 10.1089/dia.2022.0246. Epub 2022 Dec 29. Diabetes Technol Ther. 2023. PMID: 36511871 Free PMC article. Clinical Trial.
-
Glucagon orchestrates stress-induced hyperglycaemia.Diabetes Obes Metab. 2016 Jul;18(7):648-53. doi: 10.1111/dom.12668. Epub 2016 May 4. Diabetes Obes Metab. 2016. PMID: 27027662 Free PMC article. Review.
-
Multicenter Observational Study of the First-Generation Intravenous Blood Glucose Monitoring System in Hospitalized Patients.J Diabetes Sci Technol. 2015 Jul;9(4):739-50. doi: 10.1177/1932296815587939. Epub 2015 Jun 1. J Diabetes Sci Technol. 2015. PMID: 26033922 Free PMC article.
-
The effect of hypoglycaemia during hospital admission on health-related outcomes for people with diabetes: a systematic review and meta-analysis.Diabet Med. 2019 Nov;36(11):1349-1359. doi: 10.1111/dme.14115. Epub 2019 Sep 29. Diabet Med. 2019. PMID: 31441089 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
