

Dental magnetic resonance imaging: making the invisible visible
- PMID: 21787482
- PMCID: PMC3146019
- DOI: 10.1016/j.joen.2011.02.022
Dental magnetic resonance imaging: making the invisible visible
Abstract
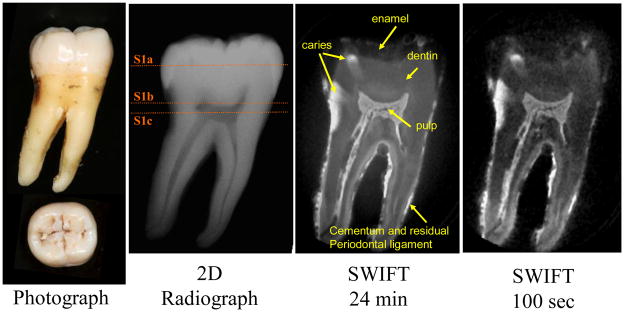
Introduction: Clinical dentistry is in need of noninvasive and accurate diagnostic methods to better evaluate dental pathosis. The purpose of this work was to assess the feasibility of a recently developed magnetic resonance imaging (MRI) technique, called SWeep Imaging with Fourier Transform (SWIFT), to visualize dental tissues.
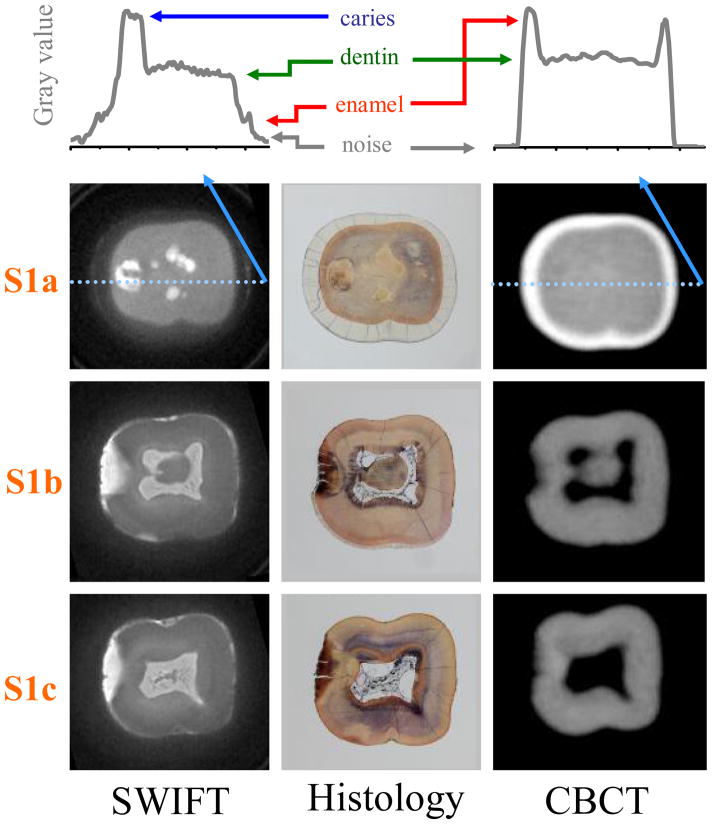
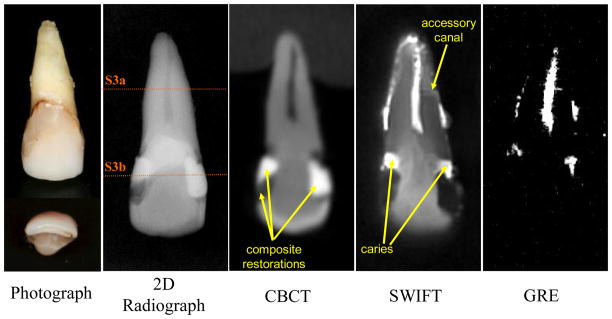
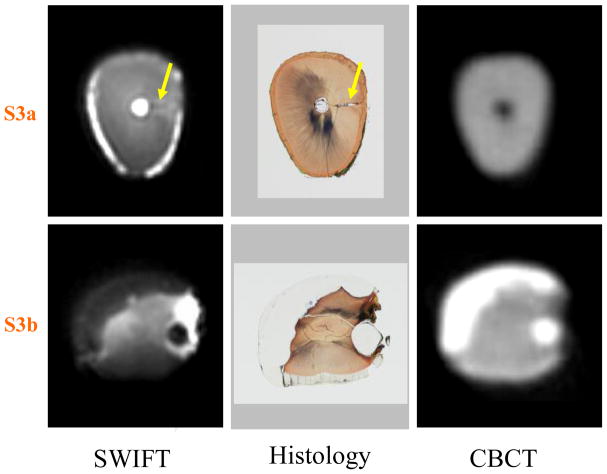
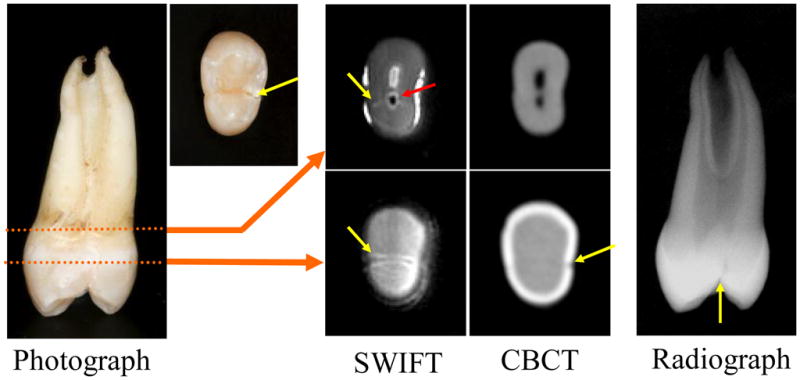
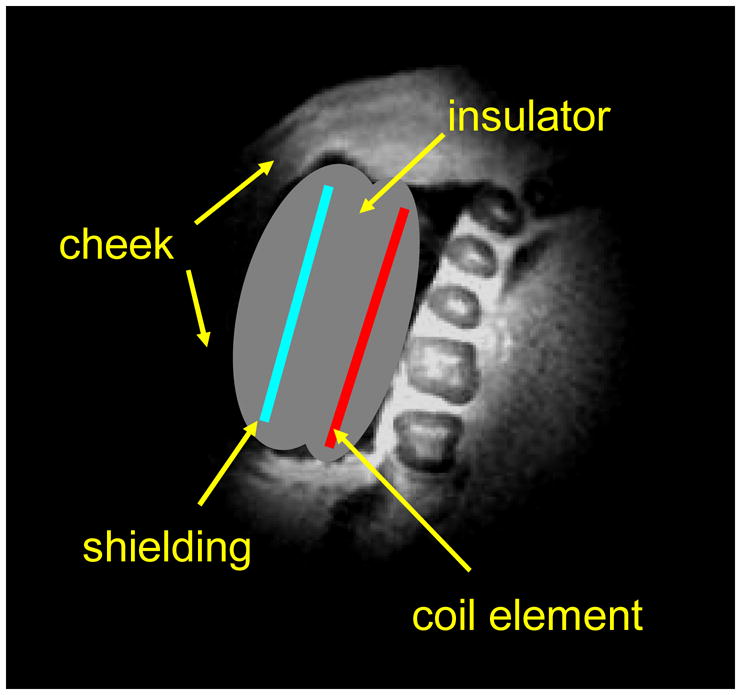
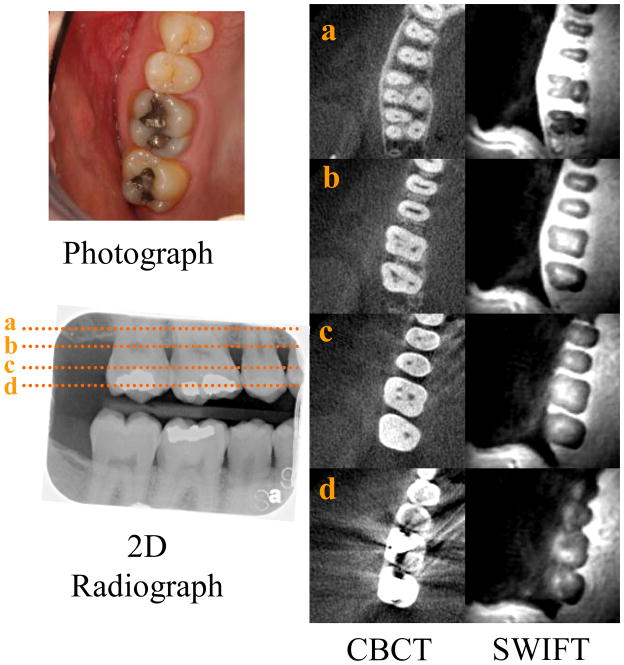
Methods: Three in vitro teeth, representing a limited range of clinical conditions of interest, imaged using a 9.4T system with scanning times ranging from 100 seconds to 25 minutes. In vivo imaging of a subject was performed using a 4T system with a 10-minute scanning time. SWIFT images were compared with traditional two-dimensional radiographs, three-dimensional cone-beam computed tomography (CBCT) scanning, gradient-echo MRI technique, and histological sections.
Results: A resolution of 100 μm was obtained from in vitro teeth. SWIFT also identified the presence and extent of dental caries and fine structures of the teeth, including cracks and accessory canals, which are not visible with existing clinical radiography techniques. Intraoral positioning of the radiofrequency coil produced initial images of multiple adjacent teeth at a resolution of 400 μm.
Conclusions: SWIFT MRI offers simultaneous three-dimensional hard- and soft-tissue imaging of teeth without the use of ionizing radiation. Furthermore, it has the potential to image minute dental structures within clinically relevant scanning times. This technology has implications for endodontists because it offers a potential method to longitudinally evaluate teeth where pulp and root structures have been regenerated.
Copyright © 2011 American Association of Endodontists. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Similar articles
-
Operative caries management in adults and children.Cochrane Database Syst Rev. 2013 Mar 28;(3):CD003808. doi: 10.1002/14651858.CD003808.pub3. Cochrane Database Syst Rev. 2013. Update in: Cochrane Database Syst Rev. 2019 Jul 24;7:CD003808. doi: 10.1002/14651858.CD003808.pub4. PMID: 23543523 Updated.
-
WITHDRAWN: Dental fillings for the treatment of caries in the primary dentition.Cochrane Database Syst Rev. 2016 Oct 17;10(10):CD004483. doi: 10.1002/14651858.CD004483.pub3. Cochrane Database Syst Rev. 2016. PMID: 27748505 Free PMC article.
-
Dental fillings for the treatment of caries in the primary dentition.Cochrane Database Syst Rev. 2009 Apr 15;(2):CD004483. doi: 10.1002/14651858.CD004483.pub2. Cochrane Database Syst Rev. 2009. Update in: Cochrane Database Syst Rev. 2016 Oct 17;10:CD004483. doi: 10.1002/14651858.CD004483.pub3. PMID: 19370602 Updated.
-
Accuracy of Magnetic Resonance Imaging in Clinical Endodontic Applications: A Systematic Review.J Endod. 2024 Apr;50(4):434-449. doi: 10.1016/j.joen.2024.01.014. Epub 2024 Jan 28. J Endod. 2024. PMID: 38290691
-
Preformed crowns for decayed primary molar teeth.Cochrane Database Syst Rev. 2015 Dec 31;2015(12):CD005512. doi: 10.1002/14651858.CD005512.pub3. Cochrane Database Syst Rev. 2015. PMID: 26718872 Free PMC article.
Cited by
-
High-resolution magnetic resonance imaging of teeth and periodontal tissues using a microscopy coil.Imaging Sci Dent. 2024 Sep;54(3):276-282. doi: 10.5624/isd.20240052. Epub 2024 Jul 17. Imaging Sci Dent. 2024. PMID: 39371311 Free PMC article.
-
Imaging studies used as aid in the diagnosis of cleidocranial dysplasia. A review.Rev Cient Odontol (Lima). 2021 Jun 21;9(2):e063. doi: 10.21142/2523-2754-0902-2021-063. eCollection 2021 Apr-Jun. Rev Cient Odontol (Lima). 2021. PMID: 38465273 Free PMC article. Review.
-
Zero-echo-time sequences in highly inhomogeneous fields.Magn Reson Med. 2025 Mar;93(3):1190-1204. doi: 10.1002/mrm.30352. Epub 2024 Oct 21. Magn Reson Med. 2025. PMID: 39428921 Free PMC article.
-
Automated tooth segmentation in magnetic resonance scans using deep learning - A pilot study.Dentomaxillofac Radiol. 2025 Jan 1;54(1):12-18. doi: 10.1093/dmfr/twae059. Dentomaxillofac Radiol. 2025. PMID: 39589897 Free PMC article.
-
Continuous SWIFT.J Magn Reson. 2012 Jul;220:26-31. doi: 10.1016/j.jmr.2012.04.016. Epub 2012 May 9. J Magn Reson. 2012. PMID: 22683578 Free PMC article.
References
-
- Longstreth WT, Jr, Phillips LE, Drangsholt M, Koepsell TD, Custer BS, Gehrels JA, et al. Dental X-rays and the risk of intracranial meningioma: a population-based case-control study. Cancer. 2004;100:1026–34. - PubMed
-
- Newton CW, Hoen MM, Goodis HE, Johnson BR, McClanahan SB. Identify and Determine the Metrics, Hierarchy, and Predictive Value of All the Parameters and/or Methods Used During Endodontic Diagnosis. J Endod. 2009;35:1635–44. - PubMed
-
- Kottoor J, Velmurugan N, Sudha R, Hemamalathi S. Maxillary first molar with seven root canals diagnosed with cone-beam computed tomography scanning: a case report. J Endod. 2010;36:915–21. - PubMed
-
- Blattner TC, George N, Lee CC, Kumar V, Yelton CD. Efficacy of cone-beam computed tomography as a modality to accurately identify the presence of second mesiobuccal canals in maxillary first and second molars: a pilot study. J Endod. 2010;36:867–70. - PubMed
-
- Hargreaves K, Law A. Cohen’s Pathways of the Pulp. 10. St. Louis, MO: Mosby Elsevier; 2010. Regenerative endodontics; pp. 602–19.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
