

Competing risks for death and cardiac transplantation in children with dilated cardiomyopathy: results from the pediatric cardiomyopathy registry
- PMID: 21788591
- PMCID: PMC3199969
- DOI: 10.1161/CIRCULATIONAHA.110.973826
Competing risks for death and cardiac transplantation in children with dilated cardiomyopathy: results from the pediatric cardiomyopathy registry
Abstract
Background: Pediatric dilated cardiomyopathy (DCM) is the leading indication for heart transplantation after 1 year of age. Risk factors by etiology at clinical presentation have not been determined separately for death and transplantation in population-based studies. Competing risks analysis may inform patient prioritization for transplantation listing.
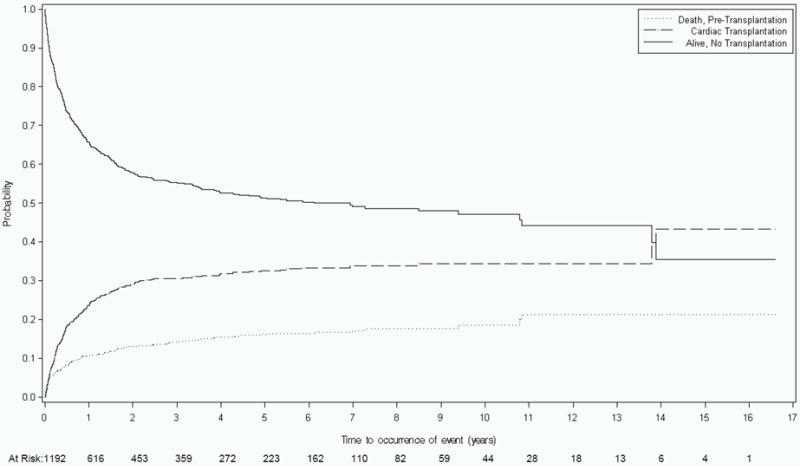
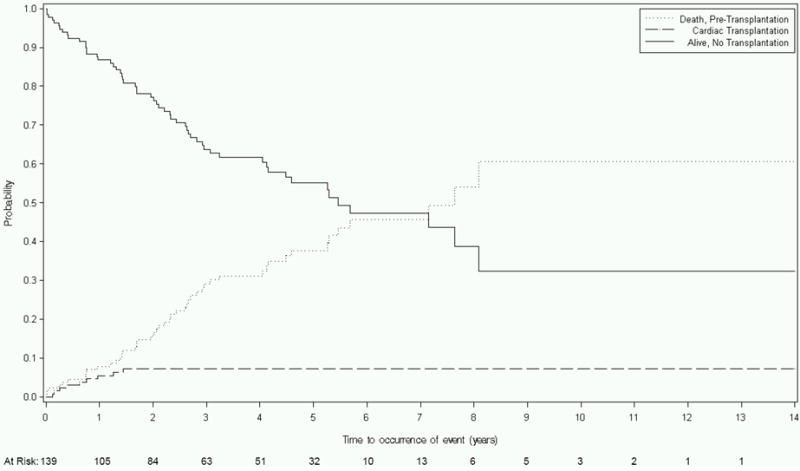
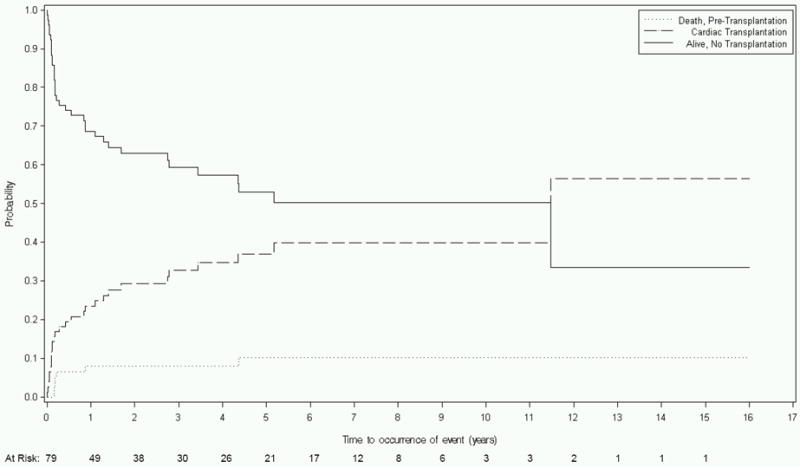
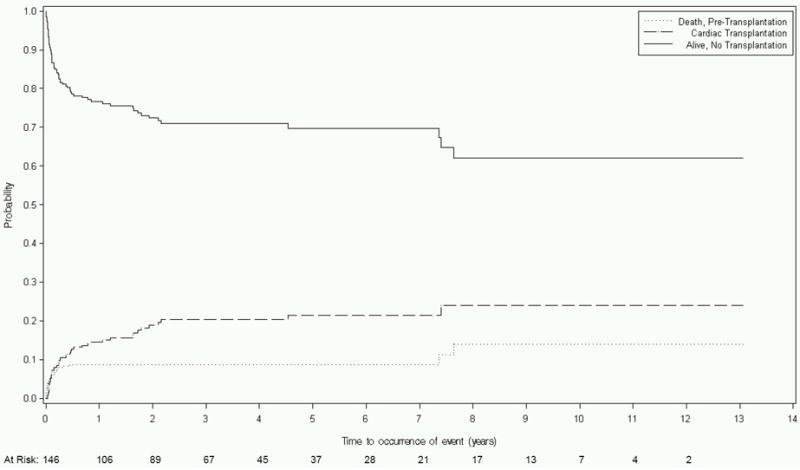
Methods and results: The Pediatric Cardiomyopathy Registry enrolled 1731 children diagnosed with DCM from 1990 to 2007. Etiologic, demographic, and echocardiographic data collected at diagnosis were analyzed with competing risks methods stratified by DCM etiology to identify predictors of death and transplantation. For idiopathic DCM (n=1192), diagnosis after 6 years of age, congestive heart failure, and lower left ventricular (LV) fractional shortening z score were independently associated with both death and transplantation equally. In contrast, increased LV end-diastolic dimension z score was associated only with transplantation, whereas lower height-for-age z score was associated only with death. For neuromuscular disease (n=139), lower LV fractional shortening was associated equally with both end points, but increased LV end-diastolic dimension was associated only with transplantation. The risks of death and transplantation were increased equally for older age at diagnosis, congestive heart failure, and increased LV end-diastolic dimension among those with myocarditis (n=272) and for congestive heart failure and decreased LV fractional shortening among those with familial DCM (n=79).
Conclusions: Risk factors for death and transplantation in children varied by DCM etiology. For idiopathic DCM, increased LV end-diastolic dimension was associated with increased transplantation risk but not mortality. Conversely, short stature was significantly related to death but not transplantation. These findings may present an opportunity to improve the transplantation selection algorithm.
Figures
References
-
- Kirk R, Edwards LB, Aurora P, Taylor DO, Christie J, Dobbels F, Kucheryavaya AY, Rahmel AO, Hertz MI. Registry of the International Society for Heart and Lung Transplantation: Eleventh Official Pediatric Heart Transplantation Report--2008. J Heart Lung Transplant. 2008;27:970–977. - PubMed
-
- Rossano JW, Kim JJ, Decker JA, Price JF, Zafar F, Graves DE, Morales DL, Heinle JS, Bozkurt B, Denfield SW, Dreyer WJ, Jefferies JL. Increasing prevalence and hospital charges in pediatric heart failure related hospitalizations in the United States: a population-based study. Circulation. 2010;122:A13740.
-
- Daubeney PE, Nugent AW, Chondros P, Carlin JB, Colan SD, Cheung M, Davis AM, Chow CW, Weintraub RG. Clinical features and outcomes of childhood dilated cardiomyopathy: results from a national population-based study. Circulation. 2006;114:2671–2678. - PubMed
-
- Towbin JA, Lowe AM, Colan SD, Sleeper LA, Orav EJ, Clunie S, Messere J, Cox GF, Lurie PR, Hsu D, Canter C, Wilkinson JD, Lipshultz SE. Incidence, causes, and outcomes of dilated cardiomyopathy in children. JAMA. 2006;296:1867–1876. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
