

Embryology and anatomy of the vesicoureteric junction with special reference to the etiology of vesicoureteral reflux
- PMID: 21789071
- PMCID: PMC3126077
- DOI: 10.1177/1756287209348985
Embryology and anatomy of the vesicoureteric junction with special reference to the etiology of vesicoureteral reflux
Abstract
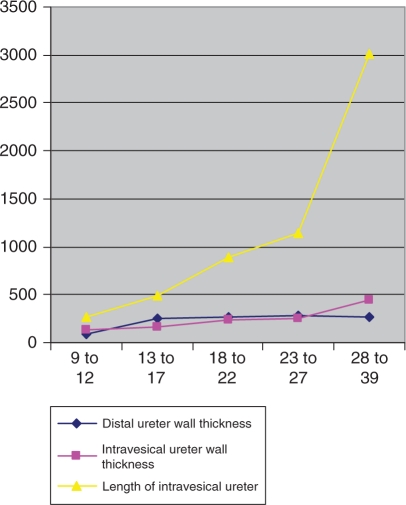
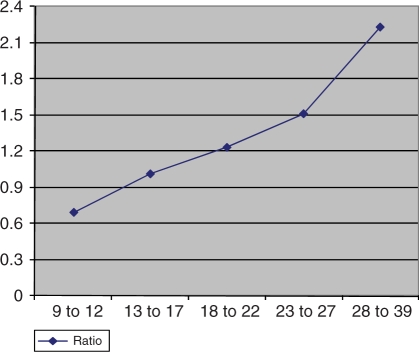
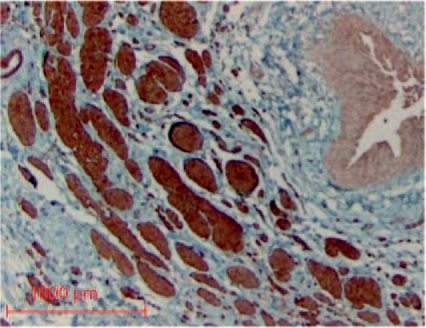
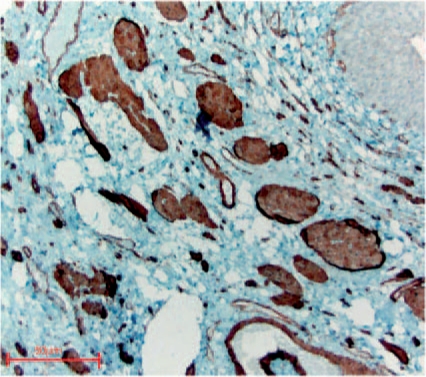
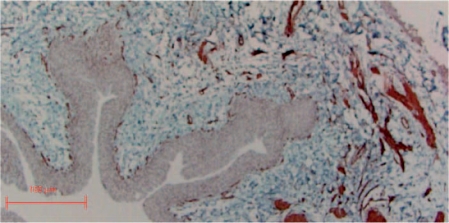
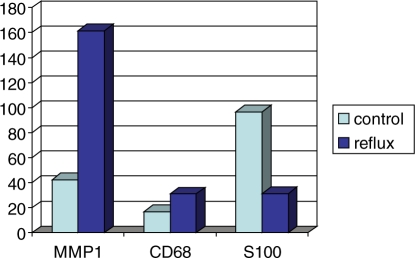
Concerning the ureterovesical junction - the region most important for the anti-reflux mechanism - there is still a lot of misunderstanding and misinterpretation with regard to normal fetal development. Data are scarce on possible causes of primary vesicoureteral reflux and on involved mechanisms of the so-called maturation process of refluxing ureteral endings. The ratio of the intravesical ureteral length to the ureteral diameter is obviously lower than assumed so far, as clearly revealed by some studies. Therefore it can be doubted that the length and course of the intravesical ureter is of sole importance in the prevention of reflux. Additionally refluxing intravesical ureteral endings present with dysplasia, atrophy, and architectural derangement of smooth muscle fibers. Besides, a pathologically increased matrix remodeling combined with deprivation of the intramural nerve supply has been confirmed. Consequently, symmetrical narrowing of the very distal ureteral smooth muscle coat creating the active valve mechanism to defend reflux is not achievable. It is apparent that primary congenital vesicoureteral reflux seems to be the result of an abnormality within the ureterovesical junction with an insufficient muscular wrap. Nature is believed to establish much more sophisticated mechanisms than the so-called passive anti-reflux mechanism. Remodeling processes within the ureterovesical junction of refluxing ureteral endings support that maturation itself is nothing else than wound or defect healing and not a restitution of a morphological normal ureterovesical junction. Lacking the nerve supply a restoration of any muscular structure can not be achieved.
Keywords: children; extracellular matrix; human fetal development; nerve supply; ureterovesical junction; vesicoureteral reflux.
Figures

Similar articles
-
Fetal development of the vesico-ureteric junction, and immunohistochemistry of the ends of refluxing ureters.J Pediatr Urol. 2005 Apr;1(2):53-9. doi: 10.1016/j.jpurol.2004.11.009. J Pediatr Urol. 2005. PMID: 18947537
-
Extracellular microenvironment and cytokine profile of the ureterovesical junction in children with vesicoureteral reflux.J Urol. 2008 Aug;180(2):694-700. doi: 10.1016/j.juro.2008.04.048. Epub 2008 Jun 13. J Urol. 2008. PMID: 18554644
-
The intravesical ureter in children with vesicoureteral reflux: a morphological and immunohistochemical characterization.J Urol. 2003 Dec;170(6 Pt 1):2423-7. doi: 10.1097/01.ju.0000097146.26432.9a. J Urol. 2003. PMID: 14634444
-
Vesicoureteral reflux and the extracellular matrix connection.Pediatr Nephrol. 2017 Apr;32(4):565-576. doi: 10.1007/s00467-016-3386-5. Epub 2016 May 2. Pediatr Nephrol. 2017. PMID: 27139901 Free PMC article. Review.
-
Physiopathology of vesico-ureteral reflux.Ital J Pediatr. 2016 Nov 29;42(1):103. doi: 10.1186/s13052-016-0316-x. Ital J Pediatr. 2016. PMID: 27899160 Free PMC article. Review.
Cited by
-
De Novo Vesicoureteral Reflux Following Ureterocele Decompression in Children: A Systematic Review and Meta-Analysis Comparing Laser Puncture versus Electrosurgical Incision Techniques.Children (Basel). 2021 Dec 24;9(1):10. doi: 10.3390/children9010010. Children (Basel). 2021. PMID: 35053634 Free PMC article. Review.
-
Association of vesicoureteral reflux and gastroesophageal reflux disease in children: A population-based study.Can Urol Assoc J. 2020 Sep;14(9):E432-E434. doi: 10.5489/cuaj.6308. Can Urol Assoc J. 2020. PMID: 32223878 Free PMC article.
-
Morphological study of the ureterovesical junction in children.J Anat. 2018 Mar;232(3):449-456. doi: 10.1111/joa.12752. J Anat. 2018. PMID: 29430696 Free PMC article.
-
Copy-number variation associated with congenital anomalies of the kidney and urinary tract.Pediatr Nephrol. 2015 Mar;30(3):487-95. doi: 10.1007/s00467-014-2962-9. Epub 2014 Oct 1. Pediatr Nephrol. 2015. PMID: 25270717
-
3-Dimensional morphometric analysis of murine bladder development and dysmorphogenesis.Dev Dyn. 2012 Mar;241(3):522-33. doi: 10.1002/dvdy.23744. Epub 2012 Jan 31. Dev Dyn. 2012. PMID: 22275180 Free PMC article.
References
-
- Anderson P., Rickwood A. (1991) Features of primary vesicoureteric reflux detected by prenatal sonography. Br J Urol 67: 267–271 - PubMed
-
- Baskin L., DiSandro M., Li Y., Li W., Hayward S., Cunha G. (2001) Mesenchymal-epithelial interactions in bladder smooth muscle development: effects of the local tissue environment. J Urol 165: 1283–1288 - PubMed
-
- Best T.M., Hunter K.D. (2000) Muscle injury and repair. Phys Med Rehabil Clin Am 11: 251–266 - PubMed
-
- Bornstein P., Sage H. (1980) Structurally distinct collagen types. Annu Rev Biochem 49: 957–1003 - PubMed
-
- Cussen L.J. (1967) Dimensions of the normal ureter in infancy and childhood. Invest Urol 5: 164–178 - PubMed
LinkOut - more resources
Full Text Sources
