

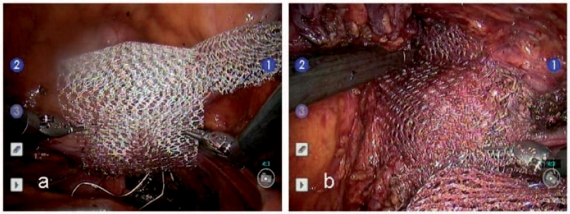
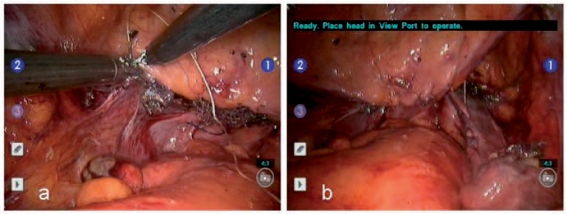
Robotic-assisted laparoscopic mesh sacrocolpopexy
- PMID: 21789075
- PMCID: PMC3126084
- DOI: 10.1177/1756287210379120
Robotic-assisted laparoscopic mesh sacrocolpopexy
Abstract
The current 'gold standard' surgical repair for apical prolapse is the abdominal mesh sacrocolpopexy. Use of a robotic-assisted laparoscopic surgical approach has been demonstrated to be feasible as a minimally invasive approach and is gaining popularity amongst pelvic floor reconstructive surgeons. Although outcome data for robotic-assisted sacrocolpopexy (RASC) is only just emerging, several small series have demonstrated anatomic and functional outcomes, as well as complication rates, comparable to those reported for open surgery. The primary advantages thus far for RASC over open surgery include decreased blood loss and shorter hospital stay.
Keywords: mesh sacrocolpopexy; pelvic prolapse; robotic surgery.
Figures
References
-
- Addison W.A., Timmons M.C. (1993) Abdominal approach to vaginal eversion. Clin Obstet Gynecol 36: 995–1004 - PubMed
-
- Addison W.A., Timmons M.C., Wall L.L., Livengood C.H., III (1989) Failed abdominal sacral colpopexy: observations and recommendations. Obstet Gynecol 74: 480–483 - PubMed
-
- Akl M.N., Long J.B., Giles D.L., Cornella J.L., Pettit P.D., Chen A.H., et al. (2009) Robotic-assisted sacrocolpopexy: technique and learning curve. Surg Endosc 23: 2390–2394 - PubMed
-
- Akladios C.Y., Dautun D., Saussine C., Baldauf J.J., Mathelin C., Wattiez A. (2010) Laparoscopic sacrocolpopexy for female genital organ prolapse: establishment of a learning curve. Eur J Obstet Gynecol Reproductive Biol 149: 218–221 - PubMed
-
- Antiphon P., Elard S., Benyoussef A., Fofana M., Yiou R., Gettman M., et al. (2004) Laparoscopic promontory sacral colpopexy: is the posterior, recto-vaginal, mesh mandatory? Eur Urol 45: 655–661 - PubMed
LinkOut - more resources
Full Text Sources
