

Dibucaine mitigates spreading depolarization in human neocortical slices and prevents acute dendritic injury in the ischemic rodent neocortex
- PMID: 21789251
- PMCID: PMC3137632
- DOI: 10.1371/journal.pone.0022351
Dibucaine mitigates spreading depolarization in human neocortical slices and prevents acute dendritic injury in the ischemic rodent neocortex
Abstract
Background: Spreading depolarizations that occur in patients with malignant stroke, subarachnoid/intracranial hemorrhage, and traumatic brain injury are known to facilitate neuronal damage in metabolically compromised brain tissue. The dramatic failure of brain ion homeostasis caused by propagating spreading depolarizations results in neuronal and astroglial swelling. In essence, swelling is the initial response and a sign of the acute neuronal injury that follows if energy deprivation is maintained. Choosing spreading depolarizations as a target for therapeutic intervention, we have used human brain slices and in vivo real-time two-photon laser scanning microscopy in the mouse neocortex to study potentially useful therapeutics against spreading depolarization-induced injury.
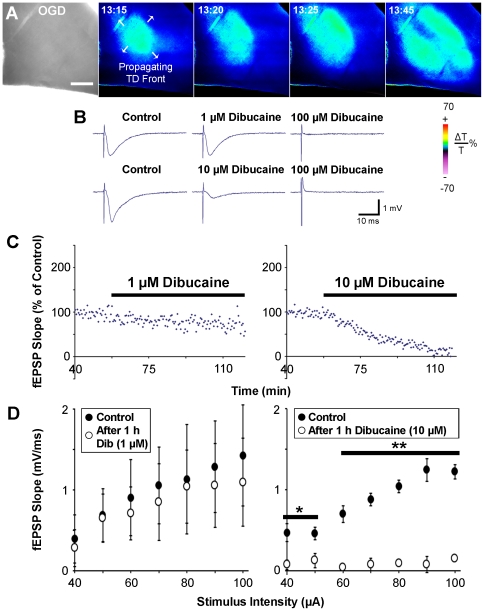
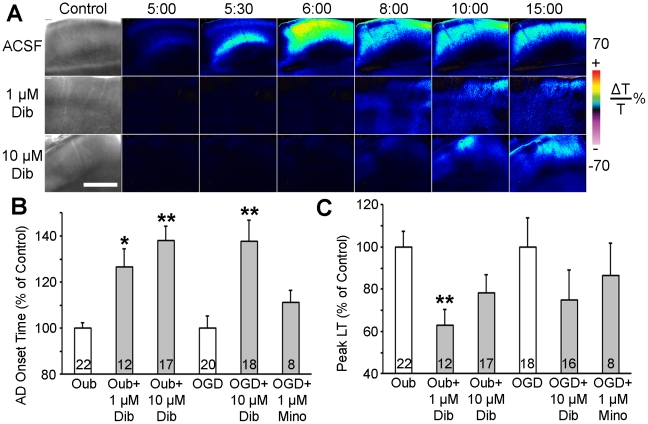
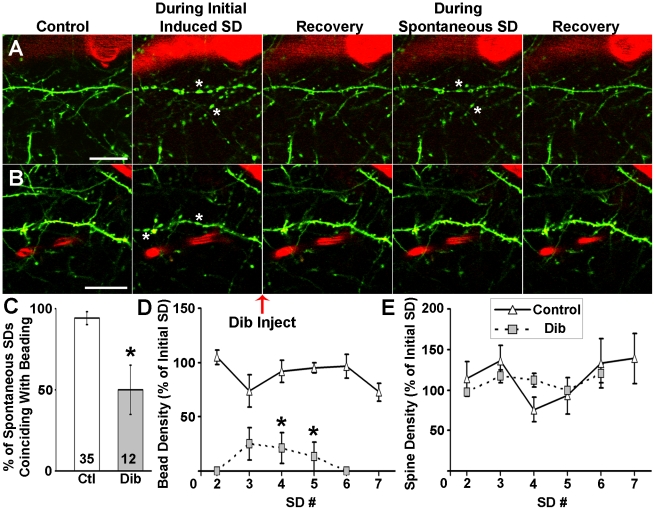
Methodology/principal findings: We have shown that anoxic or terminal depolarization, a spreading depolarization wave ignited in the ischemic core where neurons cannot repolarize, can be evoked in human slices from pediatric brains during simulated ischemia induced by oxygen/glucose deprivation or by exposure to ouabain. Changes in light transmittance (LT) tracked terminal depolarization in time and space. Though spreading depolarizations are notoriously difficult to block, terminal depolarization onset was delayed by dibucaine, a local amide anesthetic and sodium channel blocker. Remarkably, the occurrence of ouabain-induced terminal depolarization was delayed at a concentration of 1 µM that preserves synaptic function. Moreover, in vivo two-photon imaging in the penumbra revealed that, though spreading depolarizations did still occur, spreading depolarization-induced dendritic injury was inhibited by dibucaine administered intravenously at 2.5 mg/kg in a mouse stroke model.
Conclusions/significance: Dibucaine mitigated the effects of spreading depolarization at a concentration that could be well-tolerated therapeutically. Hence, dibucaine is a promising candidate to protect the brain from ischemic injury with an approach that does not rely on the complete abolishment of spreading depolarizations.
Conflict of interest statement
Figures
Similar articles
-
Potent inhibition of anoxic depolarization by the sodium channel blocker dibucaine.J Neurophysiol. 2011 Apr;105(4):1482-94. doi: 10.1152/jn.00817.2010. Epub 2011 Jan 27. J Neurophysiol. 2011. PMID: 21273307 Free PMC article.
-
Persistent astroglial swelling accompanies rapid reversible dendritic injury during stroke-induced spreading depolarizations.Glia. 2012 Nov;60(11):1709-20. doi: 10.1002/glia.22390. Epub 2012 Jul 20. Glia. 2012. PMID: 22821441 Free PMC article.
-
Imaging anoxic depolarization during ischemia-like conditions in the mouse hemi-brain slice.J Neurophysiol. 2001 Jan;85(1):414-24. doi: 10.1152/jn.2001.85.1.414. J Neurophysiol. 2001. PMID: 11152742
-
The continuum of spreading depolarizations in acute cortical lesion development: Examining Leão's legacy.J Cereb Blood Flow Metab. 2017 May;37(5):1571-1594. doi: 10.1177/0271678X16654495. Epub 2016 Jan 1. J Cereb Blood Flow Metab. 2017. PMID: 27328690 Free PMC article. Review.
-
Recording, analysis, and interpretation of spreading depolarizations in neurointensive care: Review and recommendations of the COSBID research group.J Cereb Blood Flow Metab. 2017 May;37(5):1595-1625. doi: 10.1177/0271678X16654496. Epub 2016 Jan 1. J Cereb Blood Flow Metab. 2017. PMID: 27317657 Free PMC article. Review.
Cited by
-
Rapid Neuronal Ultrastructure Disruption and Recovery during Spreading Depolarization-Induced Cytotoxic Edema.Cereb Cortex. 2020 Sep 3;30(10):5517-5531. doi: 10.1093/cercor/bhaa134. Cereb Cortex. 2020. PMID: 32483593 Free PMC article.
-
Ischemic stroke: experimental models and reality.Acta Neuropathol. 2017 Feb;133(2):245-261. doi: 10.1007/s00401-017-1667-0. Epub 2017 Jan 7. Acta Neuropathol. 2017. PMID: 28064357 Free PMC article. Review.
-
Temporo-spectral imaging of intrinsic optical signals during hypoxia-induced spreading depression-like depolarization.PLoS One. 2012;7(8):e43981. doi: 10.1371/journal.pone.0043981. Epub 2012 Aug 29. PLoS One. 2012. PMID: 22952835 Free PMC article.
-
The Role of 7,8-Dihydroxyflavone in Preventing Dendrite Degeneration in Cortex After Moderate Traumatic Brain Injury.Mol Neurobiol. 2016 Apr;53(3):1884-1895. doi: 10.1007/s12035-015-9128-z. Epub 2015 Mar 24. Mol Neurobiol. 2016. PMID: 25801526 Free PMC article.
-
Pannexin channels and ischaemia.J Physiol. 2015 Aug 15;593(16):3463-70. doi: 10.1113/jphysiol.2014.282426. Epub 2014 Dec 2. J Physiol. 2015. PMID: 25384783 Free PMC article. Review.
References
-
- Leão AA. Further observations on the spreading depression of activity in the cerebral cortex. J Neurophysiol. 1947;10:409–414. - PubMed
-
- Aitken PG, Tombaugh GC, Turner DA, Somjen GG. Similar propagation of SD and hypoxic SD-like depolarization in rat hippocampus recorded optically and electrically. J Neurophysiol. 1998;80:1514–1521. - PubMed
-
- Farkas E, Bari F, Obrenovitch TP. Multi-modal imaging of anoxic depolarization and hemodynamic changes induced by cardiac arrest in the rat cerebral cortex. Neuroimage. 2010;51:734–742. - PubMed
-
- Dreier JP. The role of spreading depression, spreading depolarization and spreading ischemia in neurological disease. Nat Med. 2011;17:439–447. - PubMed
-
- Nedergaard M, Hansen AJ. Characterization of cortical depolarizations evoked in focal cerebral ischemia. J Cereb Blood Flow Metab. 1993;13:568–574. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
