

Review
doi: 10.1111/j.1751-7133.2011.00246.x.
Epub 2011 Jul 21.
Who has advanced heart failure?: definition and epidemiology
Affiliations
- PMID: 21790965
- PMCID: PMC3857759
- DOI: 10.1111/j.1751-7133.2011.00246.x
Item in Clipboard
Review
Who has advanced heart failure?: definition and epidemiology
Congest Heart Fail.
2011 Jul-Aug.
Abstract
Summarizing current guidelines and advanced heart failure (AHF) clinical trials/registries, this review focuses on the current definition of AHF and emphasizes the secular trends in this definition over the last two decades. Further, clinical, imaging, hemodynamic, functional capacity and biomarker parameters that may aid clinicians to better recognize patients with AHF are reviewed. Finally, we review the limited data concerning the epidemiology of AHF which to date has been poorly characterized.
© 2011 Wiley Periodicals, Inc.
Figures
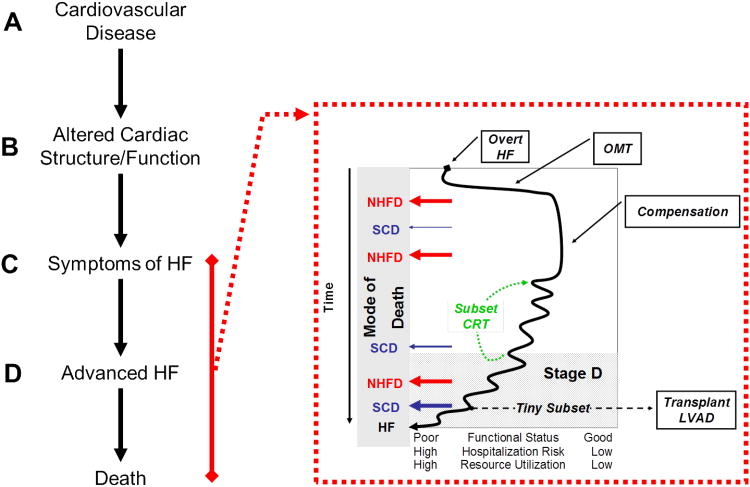
The stages in the natural history of HF clarify the relationship between
cardiovascular disease (Stage A), asymptomatic abnormalities in cardiac
structure and function (Stage B), overt symptomatic HF (Stage C) and advanced HF
(Stage D). The natural history of over HF is further characterized in the insert
where the fluctuating but progressive clinical course after HF presentation and
commencement of optimal medical therapy (OMT) or later, with cardiac
resynchronization therapy (CRT) or advanced HF therapies such as cardiac
transplantation or ventricular assist devices (LVAD) is shown. Progression to
poorer functional status associated with higher risk of hospitalization and
overall health care resource utilization occurs over time. The potential modes
of death over the course of the natural history of HF are emphasized where
patients may die of non-HF related cardiovascular or non-cardiovascular causes
(non-HF death, NHFD) or sudden cardiac death (SCD) at any time with the risk of
SCD increasing as HF worsens. Patients who avoid NHFD or SCD die of progressive
HF (HF).
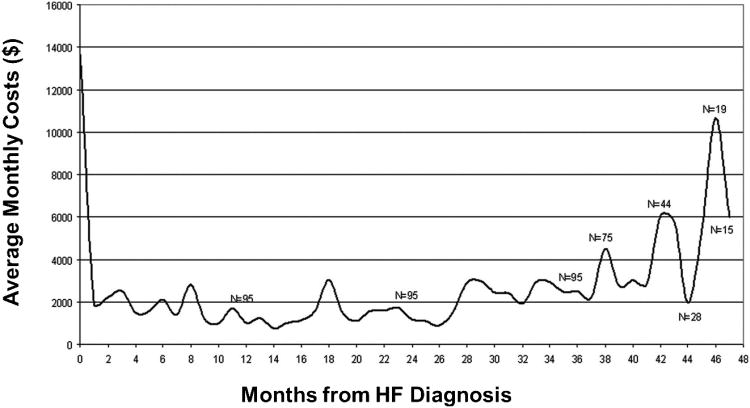
The average monthly cost of health care is shown for patients over their lifetime
after a diagnosis of HF. Note that resource utilization is most intense at the
time of diagnosis (often made during a hospitalization) and again years after
the diagnosis, where the advanced HF patient is at high risk for repeated
hospitalizations for HF or other conditions.
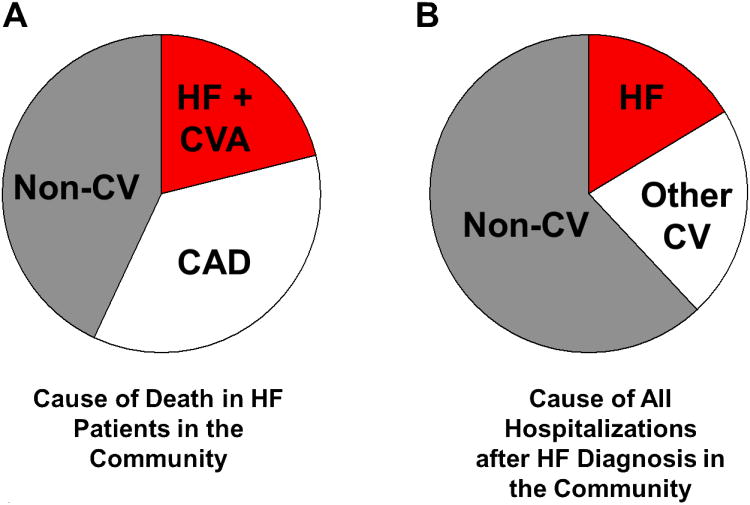
The “epidemic” of HF occurs in elderly patients where the
progression to advanced HF does not occur in isolation from a host of other
cardiovascular and non-cardiovascular comorbidities. While HF clinical trials
usually exclude patients with other cardiovascular and non-cardiovascular
comorbidities, these conditions potently contribute to mortality (A) and
hospitalizations (B)
in the community as demonstrated in studies from a community based HF
surveillance study in Olmsted County, Minnesota. In B, the cause of all
hospitalizations over the patients life after a HF diagnosis (excluding the
index HF hospitalization in patients in whom the diagnosis was made during a
hospitalization for HF) were assessed.
References
-
- Redfield MM. Heart failure--an epidemic of uncertain proportions. N Engl J Med. 2002;347(18):1442–1444. - PubMed
-
- Roger VL, Go AS, Lloyd-Jones DM, Adams RJ, Berry JD, Brown TM, Carnethon MR, Dai S, de Simone G, Ford ES, Fox CS, Fullerton HJ, Gillespie C, Greenlund KJ, Hailpern SM, Heit JA, Ho PM, Howard VJ, Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Makuc DM, Marcus GM, Marelli A, Matchar DB, McDermott MM, Meigs JB, Moy CS, Mozaffarian D, Mussolino ME, Nichol G, Paynter NP, Rosamond WD, Sorlie PD, Stafford RS, Turan TN, Turner MB, Wong ND, Wylie-Rosett J. Heart disease and stroke statistics--2011 update: a report from the American Heart Association. Circulation. 123(4):e18–e209. - PMC - PubMed
-
- Roger VL, Weston SA, Redfield MM, Hellermann-Homan JP, Killian J, Yawn BP, Jacobsen SJ. Trends in heart failure incidence and survival in a community-based population. JAMA. 2004;292(3):344–350. - PubMed
-
- Levy D, Kenchaiah S, Larson MG, Benjamin EJ, Kupka MJ, Ho KK, Murabito JM, Vasan RS. Long-term trends in the incidence of and survival with heart failure. N Engl J Med. 2002;347(18):1397–1402. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
