

Site-specific dose-response relationships for cancer induction from the combined Japanese A-bomb and Hodgkin cohorts for doses relevant to radiotherapy
- PMID: 21791103
- PMCID: PMC3161945
- DOI: 10.1186/1742-4682-8-27
Site-specific dose-response relationships for cancer induction from the combined Japanese A-bomb and Hodgkin cohorts for doses relevant to radiotherapy
Abstract
Background and purpose: Most information on the dose-response of radiation-induced cancer is derived from data on the A-bomb survivors. Since, for radiation protection purposes, the dose span of main interest is between zero and one Gy, the analysis of the A-bomb survivors is usually focused on this range. However, estimates of cancer risk for doses larger than one Gy are becoming more important for radiotherapy patients. Therefore in this work, emphasis is placed on doses relevant for radiotherapy with respect to radiation induced solid cancer.
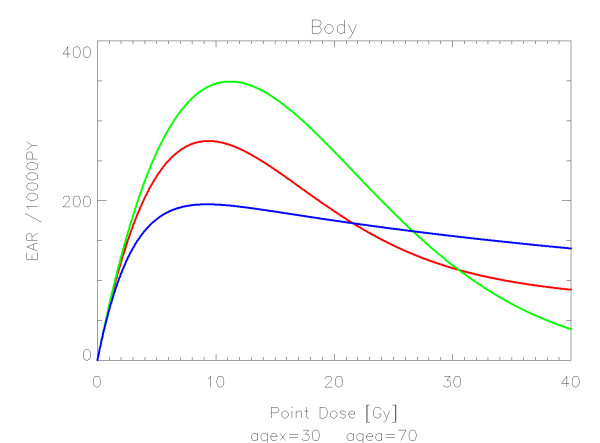
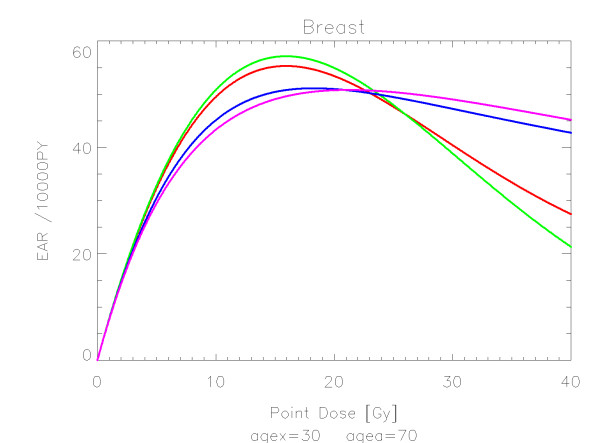
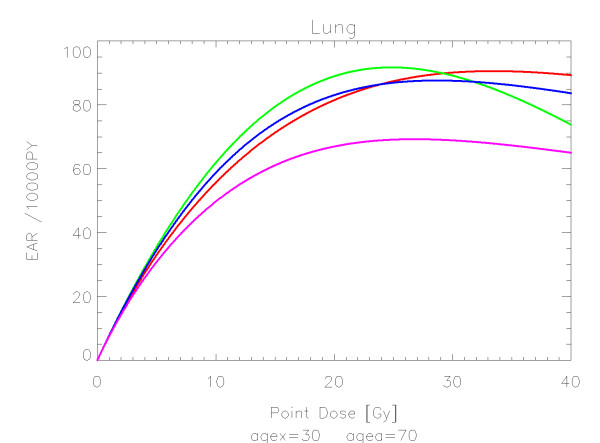
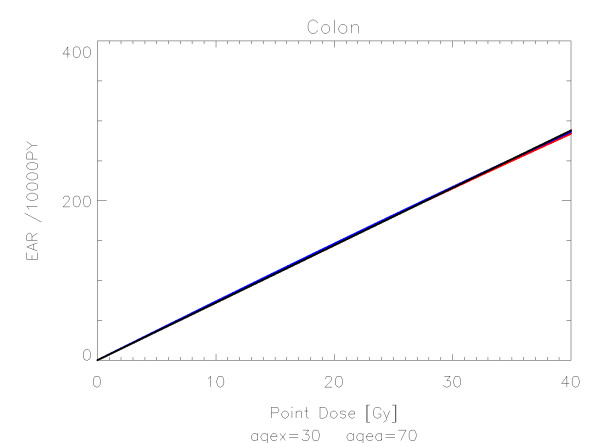
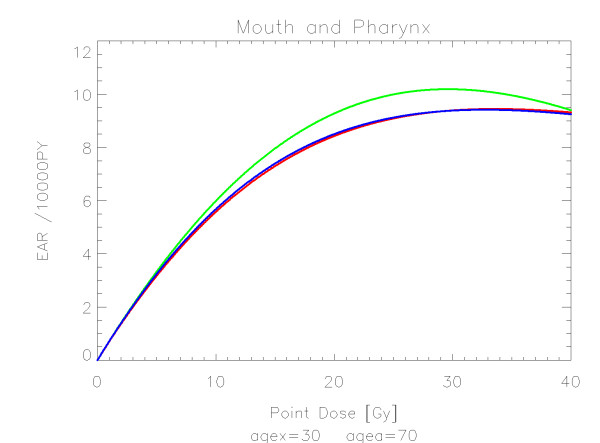
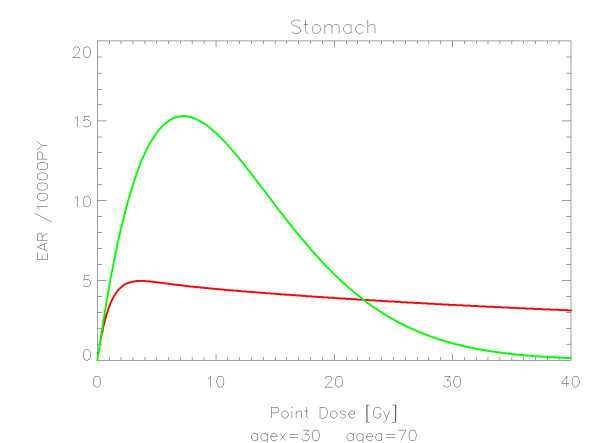
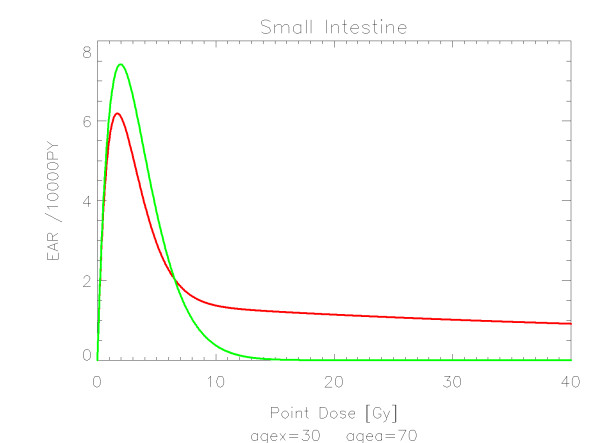
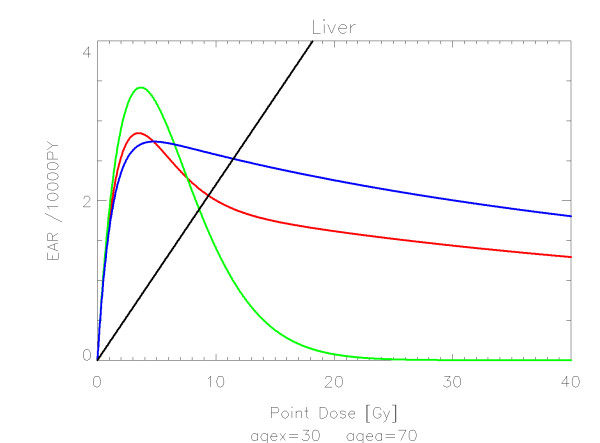
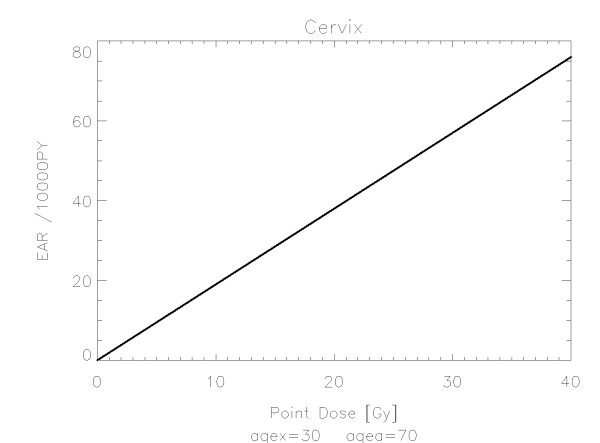
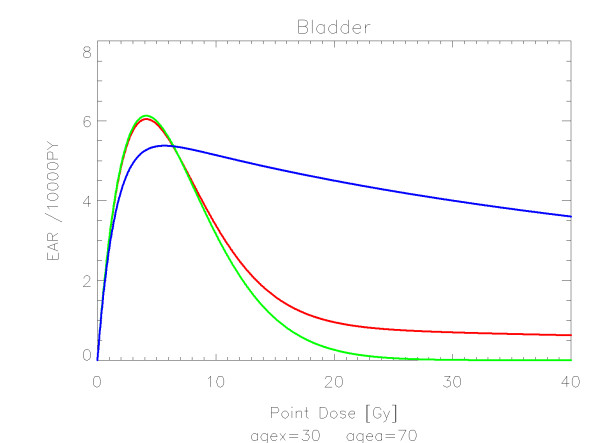
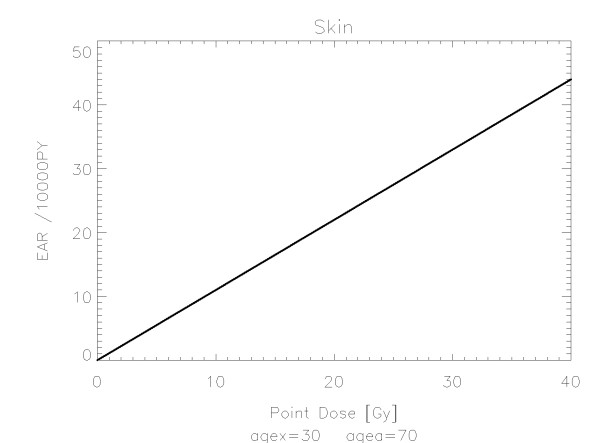
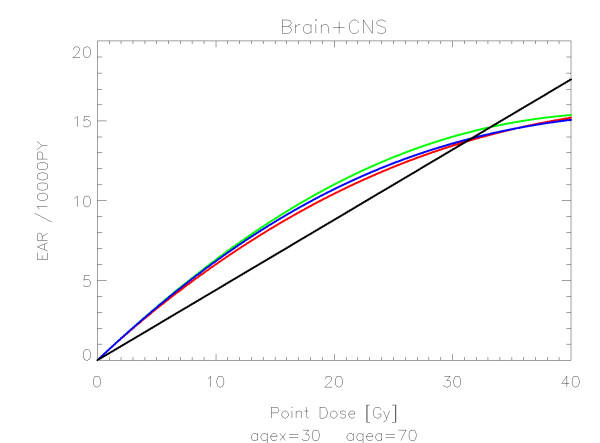
Materials and methods: For various organs and tissues the analysis of cancer induction was extended by an attempted combination of the linear-no-threshold model from the A-bomb survivors in the low dose range and the cancer risk data of patients receiving radiotherapy for Hodgkin's disease in the high dose range. The data were fitted using organ equivalent dose (OED) calculated for a group of different dose-response models including a linear model, a model including fractionation, a bell-shaped model and a plateau-dose-response relationship.
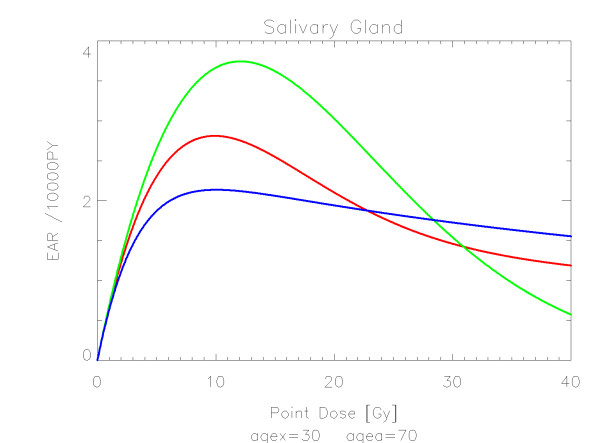
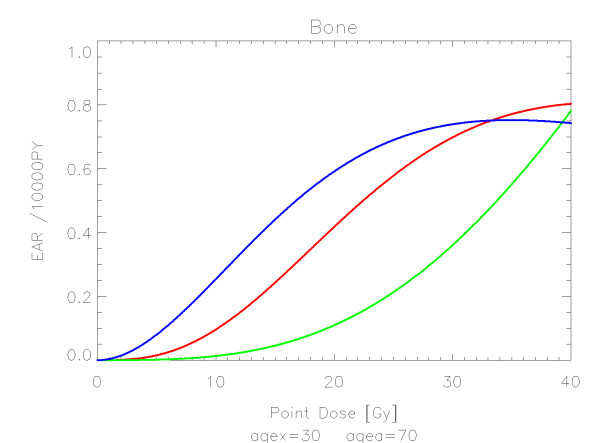
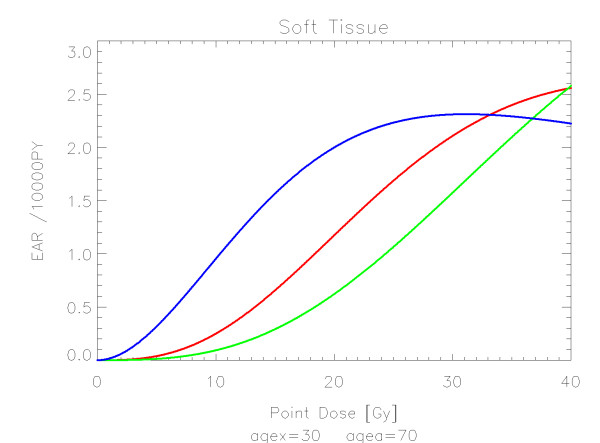
Results: The quality of the applied fits shows that the linear model fits best colon, cervix and skin. All other organs are best fitted by the model including fractionation indicating that the repopulation/repair ability of tissue is neither 0 nor 100% but somewhere in between. Bone and soft tissue sarcoma were fitted well by all the models. In the low dose range beyond 1 Gy sarcoma risk is negligible. For increasing dose, sarcoma risk increases rapidly and reaches a plateau at around 30 Gy.
Conclusions: In this work OED for various organs was calculated for a linear, a bell-shaped, a plateau and a mixture between a bell-shaped and plateau dose-response relationship for typical treatment plans of Hodgkin's disease patients. The model parameters (α and R) were obtained by a fit of the dose-response relationships to these OED data and to the A-bomb survivors. For any three-dimensional inhomogenous dose distribution, cancer risk can be compared by computing OED using the coefficients obtained in this work.
Figures
References
-
- Lindsay KA, Wheldon EG, Deehan C, Wheldon TE. Radiation carcinogenesis modelling for risk of treatment-related second tumours following radiotherapy. Br J Radiol. 2001;74(882):529–36. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
