

Elevated liver iron concentration is a marker of increased morbidity in patients with β thalassemia intermedia
- PMID: 21791471
- PMCID: PMC3208677
- DOI: 10.3324/haematol.2011.047852
Elevated liver iron concentration is a marker of increased morbidity in patients with β thalassemia intermedia
Abstract
Background: Patients with β thalassemia intermedia can have substantial iron overload, irrespectively of their transfusion status, secondary to increased intestinal iron absorption. This study evaluates whether iron overload in patients with β thalassemia intermedia is associated with morbidity.
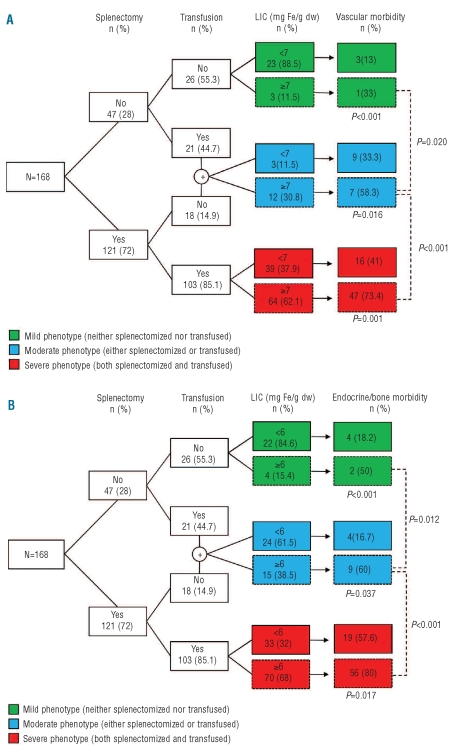
Design and methods: This was a cross-sectional study of 168 patients with β thalassemia intermedia treated at two centers in Lebanon and Italy. Data on demographics, splenectomy status, transfusion status, and presence of co-morbidities were retrieved. Laboratory values of serum ferritin, fetal and total hemoglobin levels, as well as platelet and nucleated red blood cell counts were also obtained. Iron burden was determined directly by measuring liver iron concentration using magnetic resonance imaging. Patients were subdivided according to transfusion and splenectomy status into groups with phenotypes of different severity.
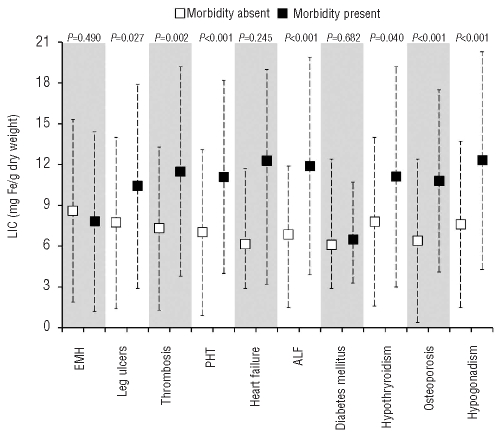
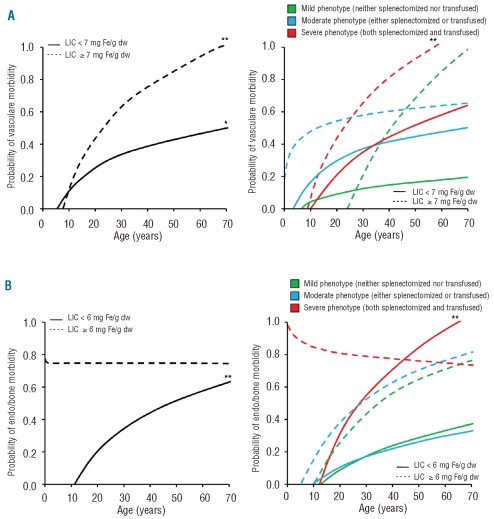
Results: The mean age of the patients was 35.2 ± 12.6 years and 42.9% of them were male. The mean liver iron concentration was 8.4 ± 6.7 mg Fe/g dry weight. On multivariate logistic regression analysis, after adjusting for age, gender, splenectomy status, transfusion status, and laboratory indices, an increase in 1 mg Fe/g dry weight liver iron concentration was independently and significantly associated with higher odds of thrombosis, pulmonary hypertension, hypothyroidism, osteoporosis, and hypogonadism. A liver iron concentration of at least 7 and at least 6 mg Fe/g dry weight were the best thresholds for discriminating the presence and absence of vascular and endocrine/bone morbidities, respectively (area under the receiver-operating characteristic curve: 0.72, P<0.001). Elevated liver iron concentration was associated with an increased rate of morbidity in patients with phenotypes of all severity, with a steeper increase in the rate of vascular morbidity being attributed to aging, and an earlier appearance of endocrine and bone disease.
Conclusions: Elevated liver iron concentration in patients with β thalassemia intermedia is a marker of increased vascular, endocrine, and bone disease.
Figures
References
-
- Steinberg MH, Forget BG, Higgs DR, Weatherall DJ. Disorders of hemoglobin: genetics pathophysiology, and clinical management. 2nd ed. Cambridge: Cambridge University Press; 2009.
-
- Taher AT, Musallam KM, Karimi M, El-Beshlawy A, Belhoul K, Daar S, et al. Overview on practices in thalassemia intermedia management aiming for lowering complication rates across a region of endemicity: the OPTIMAL CARE study. Blood. 2010;115(10):1886–92. - PubMed
-
- Taher AT, Musallam KM, Cappellini MD, Weatherall DJ. Optimal management of beta thalassaemia intermedia. Br J Haematol. 2011;152(5):512–23. - PubMed
-
- Taher A, Musallam KM, El Rassi F, Duca L, Inati A, Koussa S, et al. Levels of non-transferrin-bound iron as an index of iron overload in patients with thalassaemia intermedia. Br J Haematol. 2009;146(5):569–72. - PubMed
-
- Taher A, El Rassi F, Isma’eel H, Koussa S, Inati A, Cappellini MD. Correlation of liver iron concentration determined by R2 magnetic resonance imaging with serum ferritin in patients with thalassemia intermedia. Haematologica. 2008;93(10):1584–6. - PubMed
