

Hospital-level variation in the quality of urologic cancer surgery
- PMID: 21792864
- PMCID: PMC3273633
- DOI: 10.1002/cncr.26373
Hospital-level variation in the quality of urologic cancer surgery
Abstract
Background: Unexplained variation in outcomes after common surgeries raises concerns about the quality and appropriateness of surgical care. Understanding variation in surgical outcomes may identify processes that could affect the quality of surgical and postoperative care. The authors of this report examined hospital-level variation in outcomes after inpatient urologic oncology procedures.
Methods: Patients who underwent radical cystectomy, radical nephrectomy, and radical prostatectomy were identified from the Washington State Comprehensive Hospital Abstract Reporting System for the years 2003 through 2007. The postoperative length of stay (LOS) was measured, and LOS that exceeded the 75th percentile was classified as prolonged. The occurrence of Agency for Healthcare Quality patient safety indicators (PSIs), readmissions, and deaths also were measured. Analyses were adjusted for patient age and comorbidity in random effects, multilevel, multivariable models that assessed hospital-level outcomes.
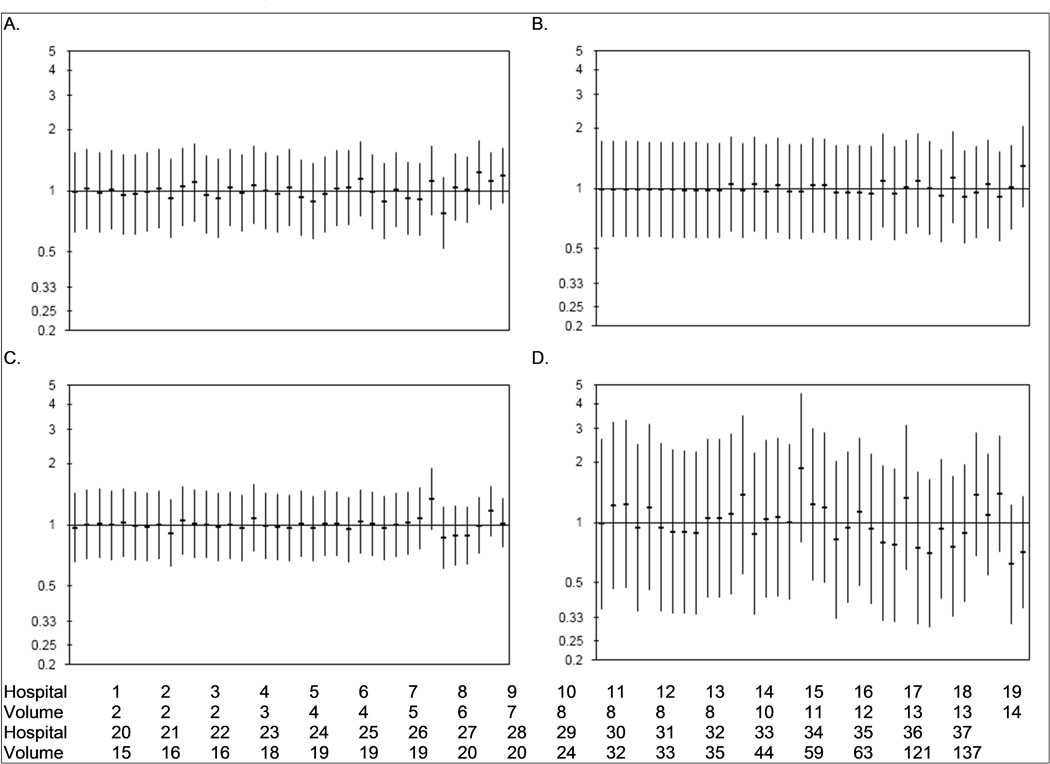
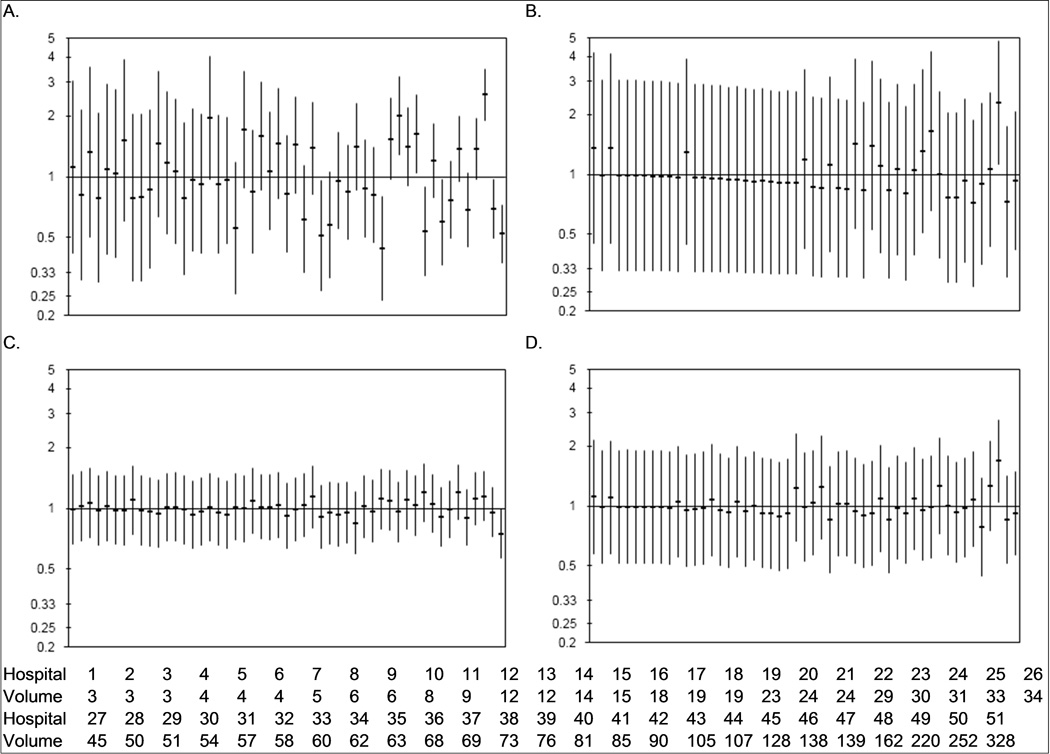
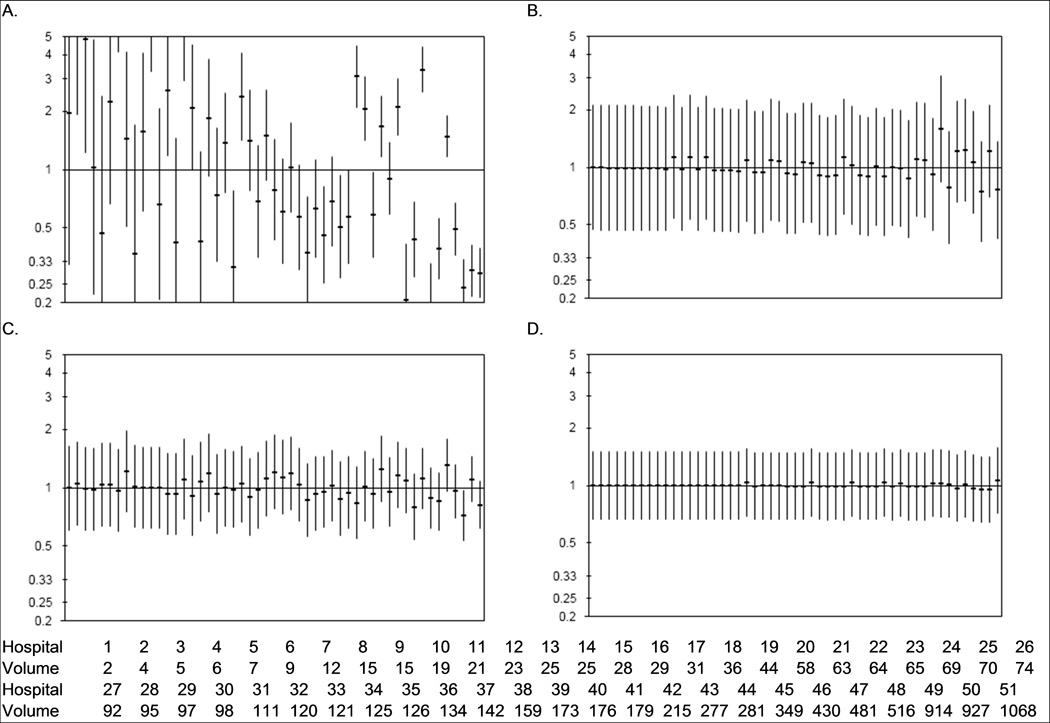
Results: The authors identified 853 patients from 37 hospitals who underwent cystectomy, 3018 patients who underwent nephrectomy from 51 hospitals, and 8228 patients who underwent prostatectomy from 51 hospitals. Complications captured by PSIs were rare. Hospital-level variation was most profound for LOS outcomes after nephrectomy and prostatectomy (variance in prolonged LOS, 8.1% and 26.7%, respectively), thromboembolic events after nephrectomy (8% of variance), and mortality after cystectomy (7.1% of variance).
Conclusions: Hospital-level variation confounds the care of urologic cancer patients in the state of Washington. The authors concluded that transparent reporting of surgical outcomes and local quality-improvement initiatives should be considered to ameliorate the observed variation and improve the quality of cystectomy, nephrectomy, and prostatectomy care.
Copyright © 2011 American Cancer Society.
Figures
References
-
- The Dartmouth atlas of health care, 1999. Chicago Ill.: American Hospital Publishing; 1999.
-
- Krupski TL, Kwan L, Afifi AA, Litwin MS. Geographic and socioeconomic variation in the treatment of prostate cancer. J Clin Oncol. 2005;23(31):7881–7888. - PubMed
-
- Lu-Yao GL, McLerran D, Wasson J, Wennberg JE. An assessment of radical prostatectomy. Time trends, geographic variation, and outcomes. The Prostate Patient Outcomes Research Team. Jama. 1993;269(20):2633–2636. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
