

In vivo 1H MRS in the assessment of the therapeutic response of breast cancer patients
- PMID: 21793075
- PMCID: PMC4226268
- DOI: 10.1002/nbm.1654
In vivo 1H MRS in the assessment of the therapeutic response of breast cancer patients
Abstract
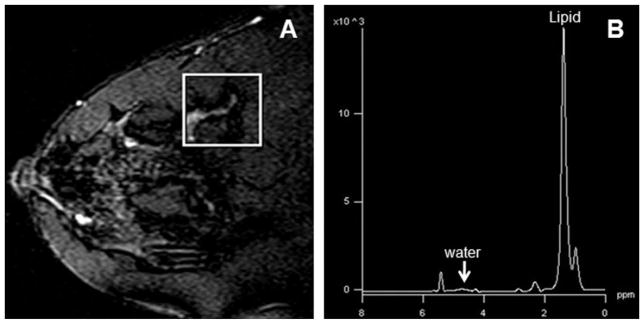
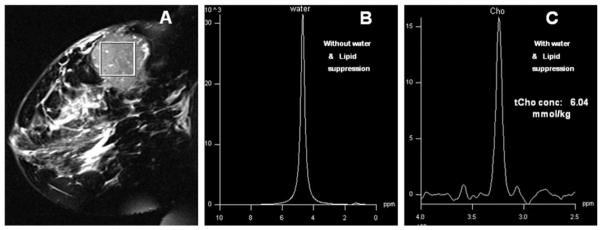
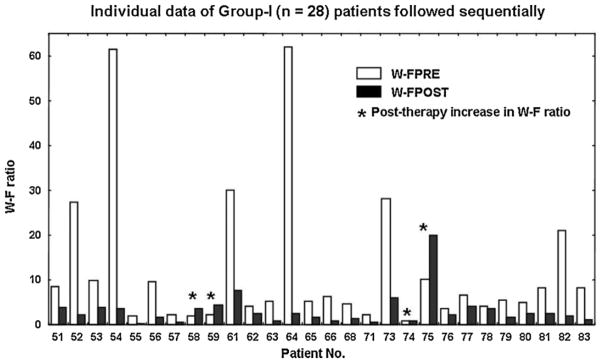
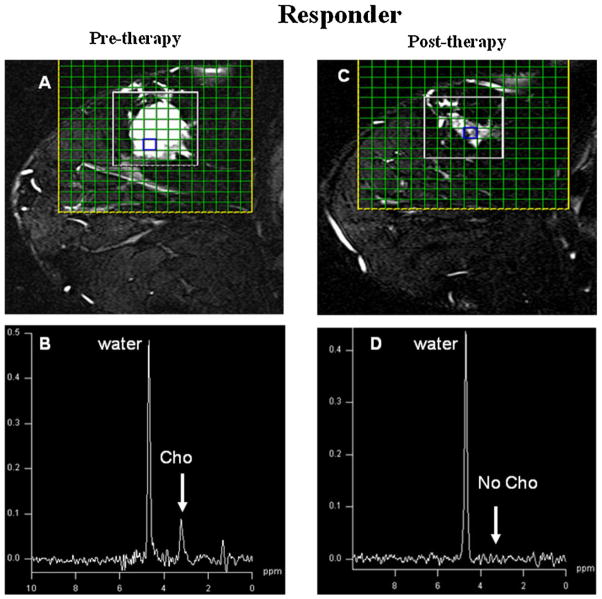
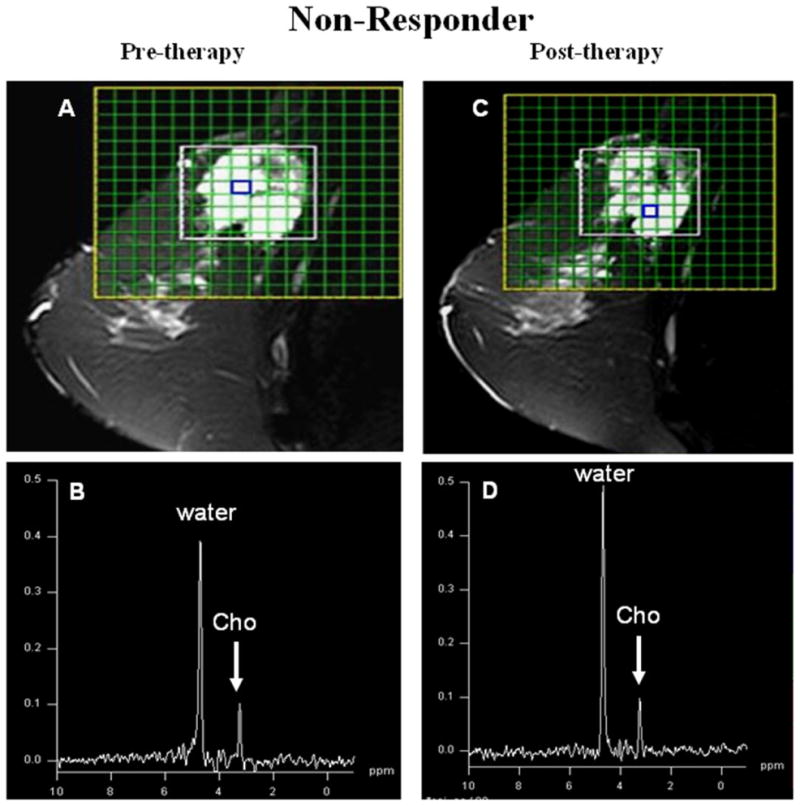
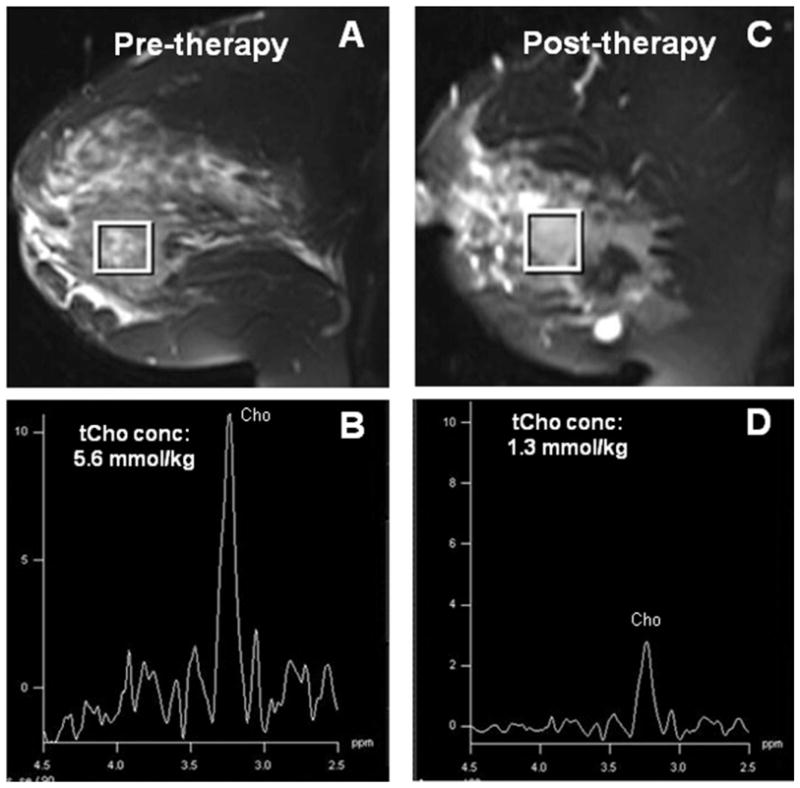
MRI and in vivo MRS have rapidly evolved as sensitive tools for diagnosis and therapeutic monitoring in cancer research. In vivo MRS provides information on tumor metabolism, which is clinically valuable in the diagnosis and assessment of tumor response to therapy for the management of women with breast diseases. Several centers complement breast MRI studies with (1)H MRS to improve the specificity of diagnosis. Malignant breast tissues show elevated water-to-fat ratio and choline-containing compounds (total choline, tCho), and any effect of therapy on tissue viability or metabolism will be manifested as changes in these levels. Sequential (1)H MRS studies have shown significantly reduced tCho levels during the course of therapy in patients who were responders. However, there are challenges in using in vivo MRS because of the relatively low sensitivity in detecting the tCho resonance with decreased lesion size or significant reduction in the tumor volume during therapy. MRS is also technically challenging because of the low signal-to-noise ratio and heterogeneous distribution of fat and glandular tissues in the breast. MRS is best utilized for the diagnosis of focal masses, most commonly seen in patients with ductal-type neoplasms; however, it has limitations in detecting nonfocal masses, such as the linear pattern of tumors seen in invasive lobular carcinoma. Further work is required to assess the clinical utility of quantitative MRS, with the goal of automation, which will reduce the subjectivity currently inherent in both qualitative and semi-quantitative MRS.
Copyright © 2011 John Wiley & Sons, Ltd.
Figures
References
-
- Garcia M, Jemal A, Ward EM, Center MM, Hao Y, Siegel RL, Thun MJ. Global Cancer Facts & Figures 2007. American Cancer Society; Atlanta, GA: 2007.
-
- NCRP (National Cancer Registry Program) An Incidence and Distribution of Cancer. Indian Council of Medical Research; New Delhi: 2001. Consolidated Report (1990–1996)
-
- Booser DJ, Hortobagayi GN. Treatment of locally advanced breast cancer. Semin Oncol. 1992;19:278–285. - PubMed
-
- Kuerer HM, Newman LA, Buzdar AU, Dhingra K, Hunt KK, Buchholz TA, Binkley SM, Strom EA, Ames FC, Ross MI, Feig BW, McNeese MD, Hortobagyi GN, Singletray SE. Pathologic tumor response in the breast following neoadjuvant chemotherapy predicts axillary lymph node status. Cancer J Sci Am. 1998;4:230–236. - PubMed
-
- Graces CA, Cance WG. Neoadjuvant chemotherapy of breast cancer. Am Surg. 2004;70:565–569. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
