

Aspirin has little additional anti-platelet effect in healthy volunteers receiving prasugrel
- PMID: 21794076
- PMCID: PMC3338354
- DOI: 10.1111/j.1538-7836.2011.04450.x
Aspirin has little additional anti-platelet effect in healthy volunteers receiving prasugrel
Abstract
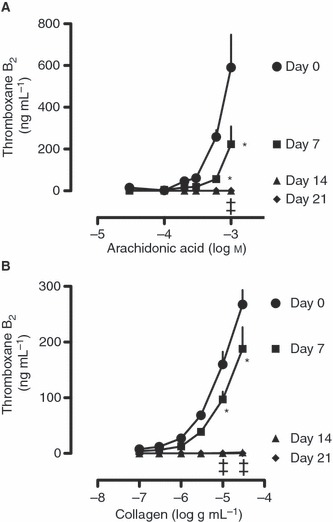
Background: Strong P2Y(12) blockade, as can be achieved with novel anti-platelet agents such as prasugrel, has been shown in vitro to inhibit both ADP and thromboxane A(2) -mediated pathways of platelet aggregation, calling into question the need for the concomitant use of aspirin.
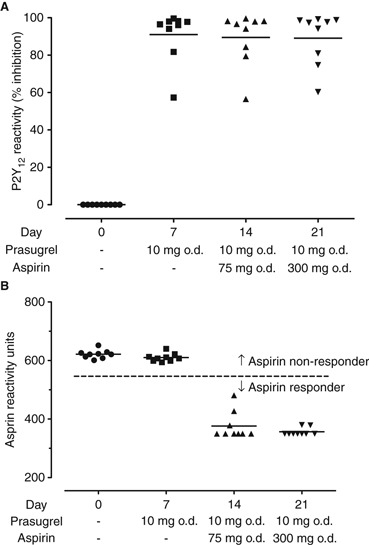
Objective: The present study investigated the hypothesis that aspirin provides little additional anti-aggregatory effect in a group of healthy volunteers taking prasugrel. STUDY PARTICIPANTS/METHODS: In all, 9 males, aged 18 to 40 years, enrolled into the 21-day study. Prasugrel was loaded at 60 mg on day 1 and maintained at 10 mg until day 21. At day 8, aspirin 75 mg was introduced and the dose increased to 300 mg on day 15. On days 0, 7, 14 and 21, platelet function was assessed by aggregometry, response to treatments was determined by VerifyNow and urine samples were collected for quantification of prostanoid metabolites.
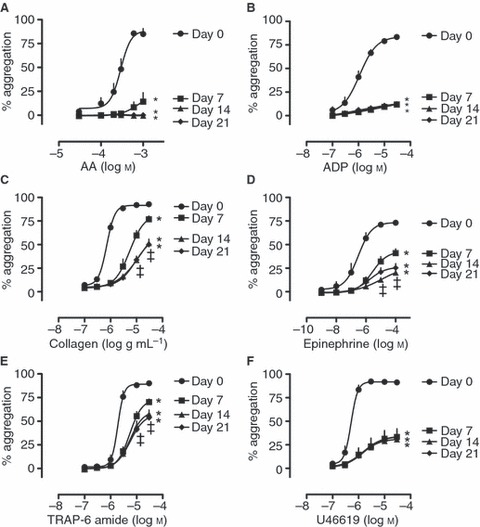
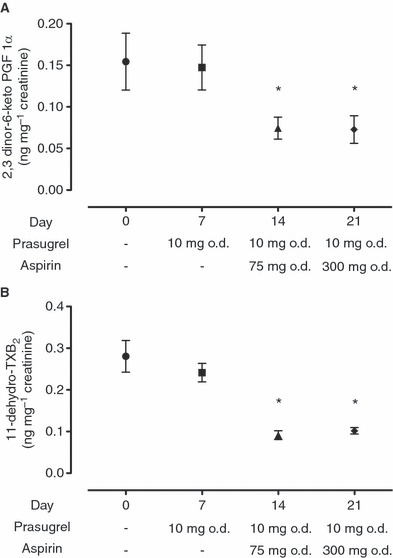
Results: At day 7, aggregation responses to a range of platelet agonists were reduced and there was only a small further inhibition of aggregation to TRAP-6, collagen and epinephrine at days 14 and 21, when aspirin was included with prasugrel. Urinary prostanoid metabolites were unaffected by prasugrel, and were reduced by the addition of aspirin, independent of dose.
Conclusions: In healthy volunteers, prasugrel produces a strong anti-aggregatory effect, which is little enhanced by the addition of aspirin. The addition of aspirin as a dual-therapy with potent P2Y(12) receptor inhibitors warrants further investigation.
© 2011 International Society on Thrombosis and Haemostasis.
Figures
References
-
- Saw J, Madsen EH, Chan S, Maurer-Spurej E. The ELAPSE (Evaluation of Long-Term Clopidogrel Antiplatelet and Systemic Anti-Inflammatory Effects) study. J Am Coll Cardiol. 2008;52:1826–33. - PubMed
-
- Mehta SR, Yusuf S, Peters RJ, Bertrand ME, Lewis BS, Natarajan MK, Malmberg K, Rupprecht H, Zhao F, Chrolavicius S, Copland I, Fox KA. Effects of pretreatment with clopidogrel and aspirin followed by long-term therapy in patients undergoing percutaneous coronary intervention: the PCI-CURE study. Lancet. 2001;358:527–33. - PubMed
-
- Anderson JL, Adams CD, Antman EM, Bridges CR, Califf RM, Casey DE, Jr, Chavey WE, 2nd, Fesmire FM, Hochman JS, Levin TN, Lincoff AM, Peterson ED, Theroux P, Wenger NK, Wright RS, Smith SC., Jr ACCF/AHA focused update incorporated into the acc/aha 2007 guidelines for the management of patients with unstable angina/non-st-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation. 2011;123:e426–579. - PubMed
-
- Li Z, Zhang G, Le Breton GC, Gao X, Malik AB, Du X. Two waves of platelet secretion induced by thromboxane A2 receptor and a critical role for phosphoinositide 3-kinases. J Biol Chem. 2003;278:30725–31. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
