

Short-term and medium-term clinical outcomes of laparoscopic-assisted and open surgery for colorectal cancer: a single center retrospective case-control study
- PMID: 21794159
- PMCID: PMC3160957
- DOI: 10.1186/1471-230X-11-85
Short-term and medium-term clinical outcomes of laparoscopic-assisted and open surgery for colorectal cancer: a single center retrospective case-control study
Abstract
Background: Laparoscopic procedure is a rapid developed technique in colorectal surgery. In this investigation we aim at assessing the diversities of short-term and medium-term clinical outcomes of laparoscopic-assisted versus open surgery for colorectal cancer.
Methods: A total number of 519 patients with non-metastatic colorectal cancer were enrolled for this study. The patients underwent either laparoscopic-assisted surgery (LAP) (n = 254) or open surgery (OP) (n = 265). Surgical techniques, perioperative managements and clinical follow-ups were standardized. Short-term perioperative data and medium-term recurrence and survival were compared and analyzed between the two groups.
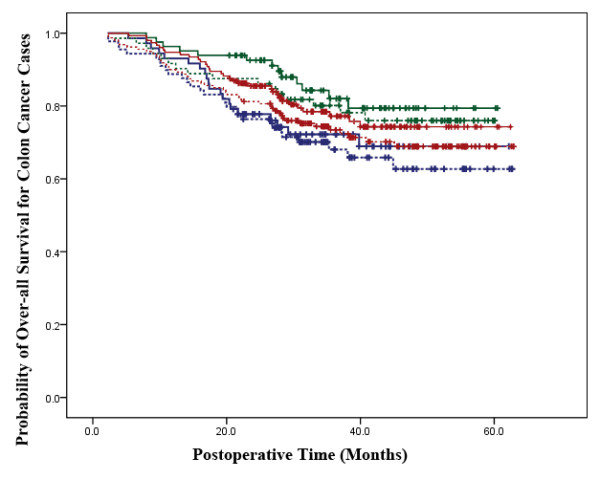
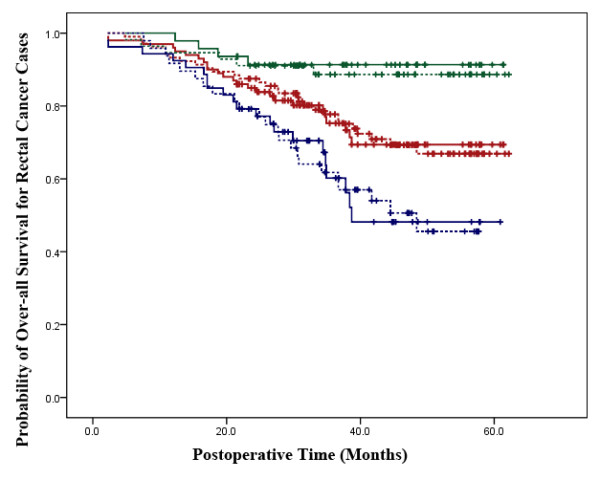
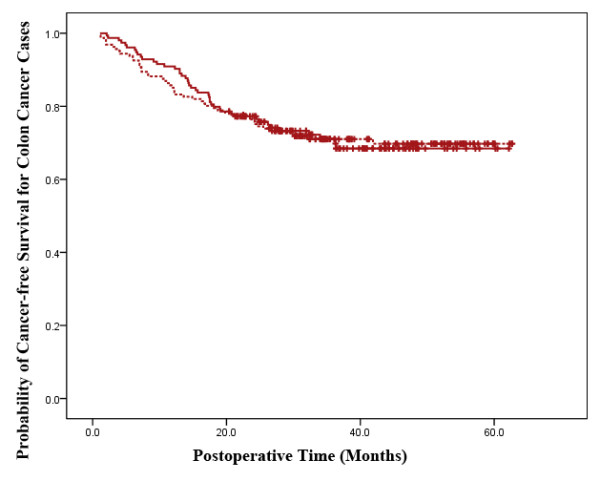
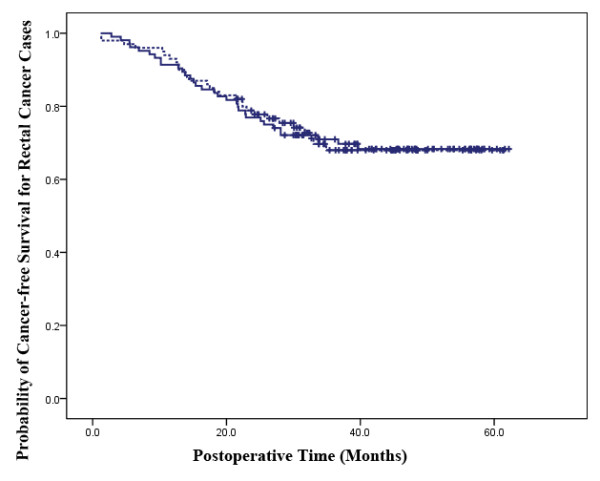
Results: There were no differences in perioperative parameters between the two groups except in regards to a trend of faster recovery in laparoscopic procedures. There was no statistically significant difference in postoperative complications, reoperation rate, or perioperative mortality. Statistically significant differences in a faster return of gastrointestinal function and shorter hospital stay were identified in favor of laparoscopic-assisted resection. In colon and rectal cancer cases separately, the overall survival, cancer-free survival and recurrence rate were similar in two groups. There was also no tendency of significant differences in overall survival, cancer-free survival and recurrence in stage I-II and stage III patients in two cancer categories between the two groups, respectively. pT, lymph node metastasis, and clinical stage were independent predictors of overall death risk, while pT, pN, lymph node metastasis and clinical stage were found to be the independent predictors of recurrence risk in enrolled patients database.
Conclusions: Laparoscopic-assisted procedure has more benefits on postoperative recovery, while has the same effects on medium-term recurrence and survival compared with open surgery in the treatment of non-metastatic colorectal cancer.
Figures
References
-
- NCCN clinical practice guidelines oncology. http://www.nccn.org/professionals/physician_gls/f_guidelines.asp
-
- Jacobs M, Verdeja JC, Goldstein HS. Minimally invasive colon resection (laparoscopic colectomy) Surg Laparosc Endosc. 1991;1:144–150. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
