

Diagnostic performance of fractional excretion of urea in the evaluation of critically ill patients with acute kidney injury: a multicenter cohort study
- PMID: 21794161
- PMCID: PMC3387621
- DOI: 10.1186/cc10327
Diagnostic performance of fractional excretion of urea in the evaluation of critically ill patients with acute kidney injury: a multicenter cohort study
Abstract
Introduction: Several factors, including diuretic use and sepsis, interfere with the fractional excretion of sodium, which is used to distinguish transient from persistent acute kidney injury (AKI). These factors do not affect the fractional excretion of urea (FeUrea). However, there are conflicting data on the diagnostic accuracy of FeUrea.
Methods: We conducted an observational, prospective, multicenter study at three ICUs in university hospitals. Unselected patients, except those with obstructive AKI, were admitted to the participating ICUs during a six-month period. Transient AKI was defined as AKI caused by renal hypoperfusion and reversal within three days. The results are reported as medians (interquartile ranges).
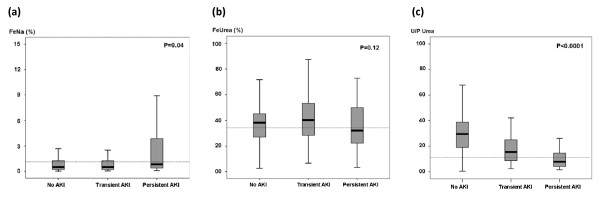
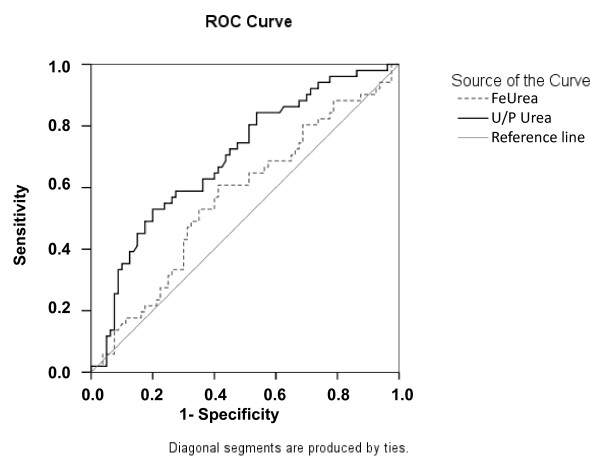
Results: A total of 203 patients were included. According to our definitions, 67 had no AKI, 54 had transient AKI and 82 had persistent AKI. FeUrea was 39% (28 to 40) in the no-AKI group, 41% (29 to 54) in the transient AKI group and 32% (22 to 51) in the persistent AKI group (P = 0.12). FeUrea was of little help in distinguishing transient AKI from persistent AKI, with the area under the receiver operating characteristic curve being 0.59 (95% confidence interval, 0.49 to 0.70; P = 0.06). Sensitivity was 63% and specificity was 54% with a cutoff of 35%. In the subgroup of patients receiving diuretics, the results were similar.
Conclusions: FeUrea may be of little help in distinguishing transient AKI from persistent AKI in critically ill patients, including those receiving diuretic therapy. Additional studies are needed to evaluate alternative markers or strategies to differentiate transient from persistent AKI.
Figures
References
-
- Brivet FG, Kleinknecht DJ, Loirat P, Landais JP. French Study Group on Acute Renal Failure. Acute renal failure in intensive care units-causes, outcome, and prognostic factors of hospital mortality: a prospective, multicenter study. Crit Care Med. 1996;24:192–198. doi: 10.1097/00003246-199602000-00003. - DOI - PubMed
-
- Uchino S, Kellum JA, Bellomo R, Doig GS, Morimatsu H, Morgera S, Schetz M, Tan I, Bouman C, Macedo E, Gibney N, Tolwani A, Ronco C. Beginning and Ending Supportive Therapy for the Kidney (BEST Kidney) Investigators. Acute renal failure in critically ill patients: a multinational, multicenter study. JAMA. 2005;294:813–818. doi: 10.1001/jama.294.7.813. - DOI - PubMed
-
- Lameire N, Van Biesen W, Vanholder R. Acute renal failure. Lancet. 2005;365:417–430. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
