

Risk factors for epilepsy in children with neonatal encephalopathy
- PMID: 21796017
- PMCID: PMC3189270
- DOI: 10.1203/PDR.0b013e31822f24c7
Risk factors for epilepsy in children with neonatal encephalopathy
Abstract
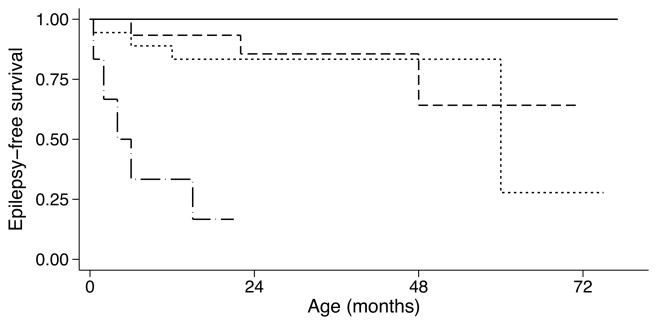
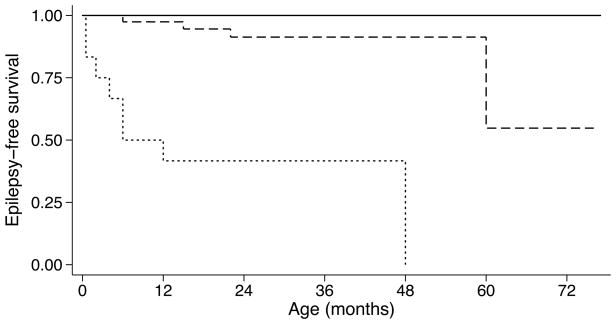
We examined neonatal predictors of epilepsy in term newborns with neonatal encephalopathy (NE) by studying children enrolled in a longitudinal, single center cohort study. Clinical data were obtained through chart review, and MRI was performed in the neonatal period. We administered a seizure questionnaire to parents of children aged ≥ 12 mo (range, 12 mo to 16.5 y) to determine the outcome of epilepsy. The association between clinical predictors and time to onset of epilepsy was assessed using Cox proportional hazards regression. Thirteen of 129 children developed epilepsy: all had neonatal seizures and brain injury on neonatal MRI. Of the newborns with neonatal seizures, 25% (15.8/1000 person-years) developed epilepsy, with the highest hazard ratios (HRs) in the newborns with status epilepticus (HR, 35.8; 95% CI, 6.5-196.5). Children with severe or near-total brain injury were more likely to develop epilepsy compared with those with only mild or moderate injury (HR, 5.5; 95% CI, 1.8-16.8). In a multivariable analysis adjusting for degree of encephalopathy and severe/near-total brain injury, status epilepticus was independently associated with epilepsy. These data add to information regarding epilepsy pathogenesis and further aid clinicians to counsel parents regarding the likelihood that a newborn with NE will develop epilepsy.
Figures
References
-
- Thornberg E, Thiringer K, Odeback A, Milsom I. Birth asphyxia: incidence, clinical course and outcome in a Swedish population. Acta Paediatr. 1995;84:927–932. - PubMed
-
- Graham EM, Ruis KA, Hartman AL, Northington FJ, Fox HE. A systematic review of the role of intrapartum hypoxia-ischemia in the causation of neonatal encephalopathy. Am J Obstet Gynecol. 2008;199:587–595. - PubMed
-
- Kurinczuk JJ, White-Koning M, Badawi N. Epidemiology of neonatal encephalopathy and hypoxic-ischaemic encephalopathy. Early Hum Dev. 2010;86:329–338. - PubMed
-
- Pisani F, Orsini M, Braibanti S, Copioli C, Sisti L, Turco EC. Development of epilepsy in newborns with moderate hypoxic-ischemic encephalopathy and neonatal seizures. Brain Dev. 2009;31:64–68. - PubMed
-
- Belet N, Belet U, Incesu L, Uysal S, Ozinal S, Keskin T, Sunter AT, Kucukoduk S. Hypoxic-ischemic encephalopathy: C\correlation of serial MRI and outcome. Pediatr Neurol. 2004;31:267–274. - PubMed
