

Hip-spine relations and sagittal balance clinical consequences
- PMID: 21796392
- PMCID: PMC3175930
- DOI: 10.1007/s00586-011-1937-9
Hip-spine relations and sagittal balance clinical consequences
Abstract
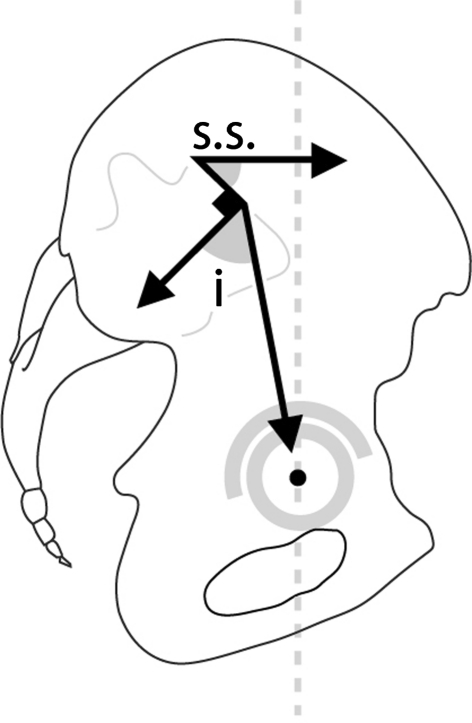
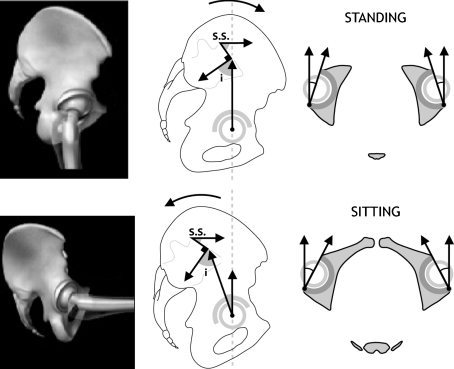
Introduction: The role of the pelvic area in sagittal balance is evident for spinal surgeons, but the influence of the coxofemoral joint is underestimated and inadequately explained by conventional imagery. Comprehensive analysis of the pelvic and subpelvic sectors as part of the sagittal, frontal and cross-sectional balance of the trunk sheds new light on some spinal diseases and their relation to the pelvis.
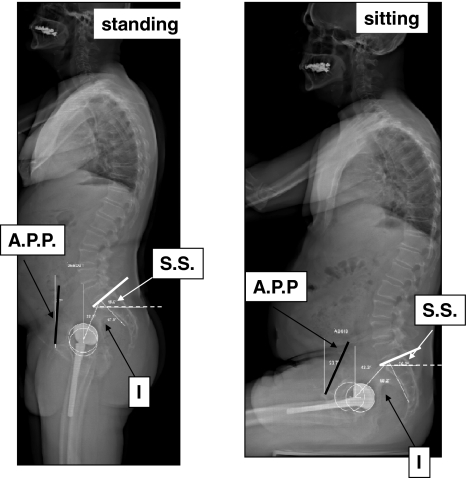
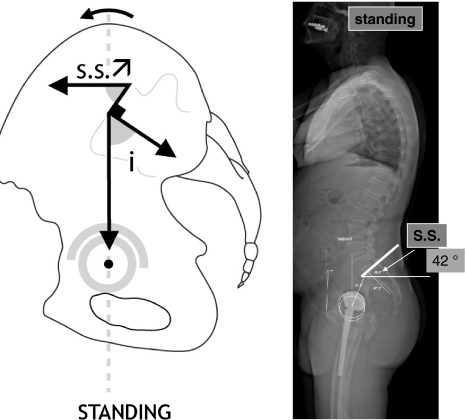
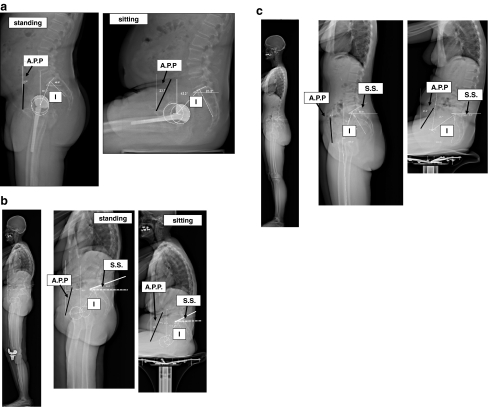
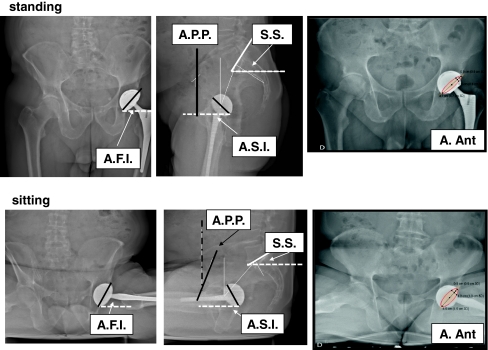
Methods: This analysis, based on innovative radiologic methods as the EOS(®) technology but also on a new look at conventional imaging makes it possible to better analyze standing lateral images and seated images.
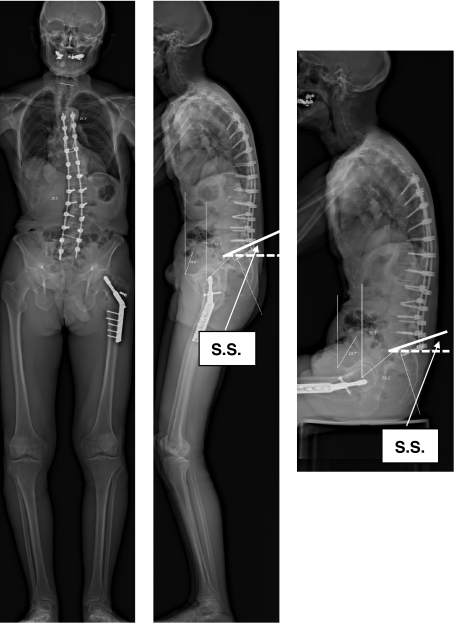
Results: Disturbances can come from atypical morphotypes or from unusual postures as in aging spine. The measurement of available extension and the concept of available flexion provide new information regarding individual's adaptation to the imbalance induced by disorders of the spine or lower limbs.
Conclusion: A comprehensive assessment of each patient and in particular of the complex comprising the spine and the pelvis, is essential for understanding each individual's adaptation to the imbalance induced by disorders of the spine or lower limbs.
Figures









References
-
- Jackson RP, McManus AC. Radiographic analysis of sagittal plane alignment and balance in standing volunteers and patients with low back pain matched for age, sex, and size. A prospective controlled clinical study. Spine (Phila Pa 1976) 1994;19(14):1611–1618. doi: 10.1097/00007632-199407001-00010. - DOI - PubMed
-
- Padgett DE, Warashina H (2004) The unstable total hip replacement. Clin Orthop Relat Res 420(1):72–79 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
