

Beyond the prescription: medication monitoring and adverse drug events in older adults
- PMID: 21797831
- PMCID: PMC3940362
- DOI: 10.1111/j.1532-5415.2011.03500.x
Beyond the prescription: medication monitoring and adverse drug events in older adults
Abstract
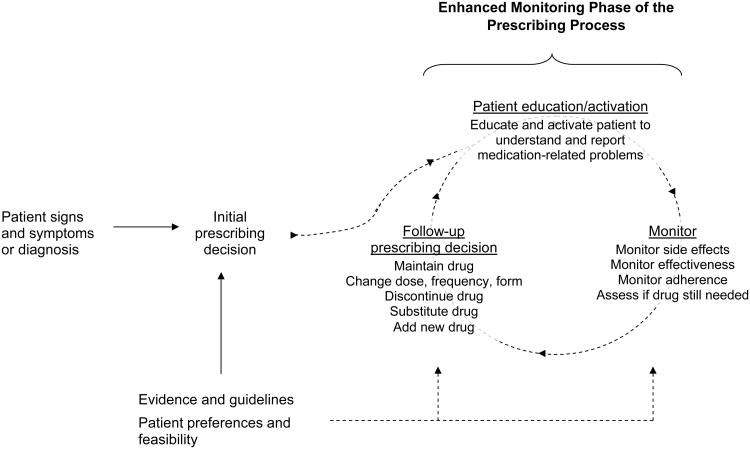
Whether a person will suffer harm from a medication or how severe that harm will be is difficult to predict precisely. As a result, many adverse drug events (ADEs) occur in patients in whom it was reasonable to believe that the drug's benefits exceeded its risks. Improving safety and reducing the burden of ADEs in older adults requires addressing this uncertainty by not only focusing on the appropriateness of the initial prescribing decision, but also by detecting and mitigating adverse events once they have started to occur. Such enhanced monitoring of signs, symptoms, and laboratory parameters can determine whether an adverse event has only mild and short-term consequences or major long-term effects on morbidity and mortality. Although current medication monitoring practices are often suboptimal, several strategies can be leveraged to improve the quality and outcomes of monitoring. These strategies include using health information technology to link pharmacy and laboratory data, prospective delineation of risk, and patient outreach and activation, all within a framework of team-based approaches to patient management. Although many of these strategies are theoretically possible now, they are poorly used and will be difficult to implement without a significant restructuring of medical practice. An enhanced focus on medication monitoring will also require a new conceptual framework to re-engineer the prescribing process. With this approach, prescribing quality does not hinge on static attributes of the initial prescribing decision but entails a dynamic process in which the benefits and harms of drugs are actively monitored, managed, and reassessed over time.
© 2011, Copyright the Authors. Journal compilation © 2011, The American Geriatrics Society.
Conflict of interest statement
Disclosure: The authors have no conflicts of interest with subjects discussed in this manuscript.
Opinions expressed in this manuscript are those of the authors and do not necessarily reflect the position of the U.S. Government or Department of Veterans Affairs.
Figures
References
-
- Hanlon JT, Schmader KE, Ruby CM, Weinberger M. Suboptimal prescribing in older inpatients and outpatients. J Am Geriatr Soc. 2001;49(2):200–209. - PubMed
-
- Roden DM. Chapter 5. Principles of Clinical Pharmacology. In: Fauci AS, Braunwald E, Kasper DL, et al., editors. Harrison's Online [Harrison's principles of internal medicine online edition] New York: McGraw Hill;
-
- Hilmer SN, Ford GA. General Principles of Pharmacology. In: Halter JB, Ouslander JG, Tinetti ME, Studenski S, High KP, Asthana S, editors. Hazzard's Geriatric Medicine and Gerontology, version 6e. New York: McGraw-Hill;
-
- Pompei P, editor. Geriatrics Review Syllabus: A Core Curriculum in Geriatric Medicine. Sixth. Fry Communications; Pharmacotherapy.
-
- Avorn J. Improving drug use in elderly patients: getting to the next level. JAMA. 2001 Dec 12;286(22):2866–2868. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
