

Quantitative radiologic criteria for the diagnosis of lumbar spinal stenosis: a systematic literature review
- PMID: 21798008
- PMCID: PMC3161920
- DOI: 10.1186/1471-2474-12-175
Quantitative radiologic criteria for the diagnosis of lumbar spinal stenosis: a systematic literature review
Abstract
Background: Beside symptoms and clinical signs radiological findings are crucial in the diagnosis of lumbar spinal stenosis (LSS). We investigate which quantitative radiological signs are described in the literature and which radiological criteria are used to establish inclusion criteria in clinical studies evaluating different treatments in patients with lumbar spinal stenosis.
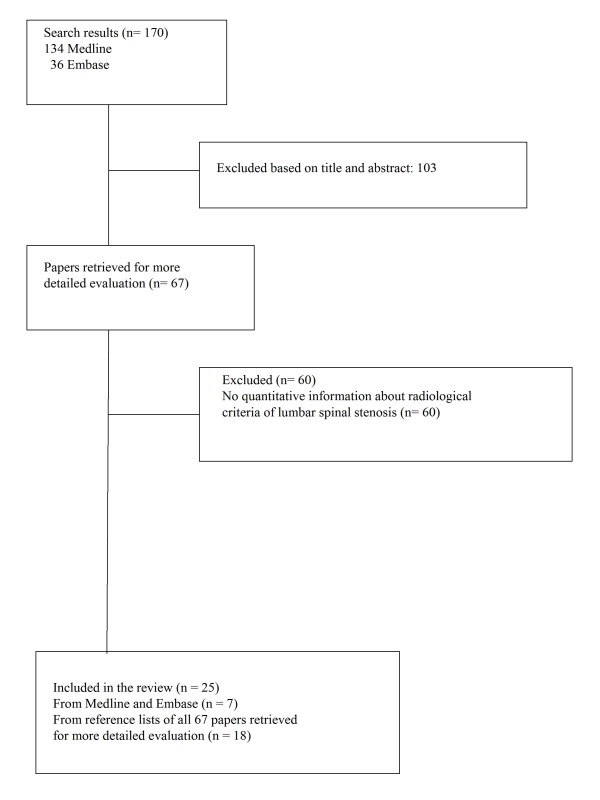
Methods: A literature search was performed in Medline, Embase and the Cochrane library to identify papers reporting on radiological criteria to describe LSS and systematic reviews investigating the effects of different treatment modalities.
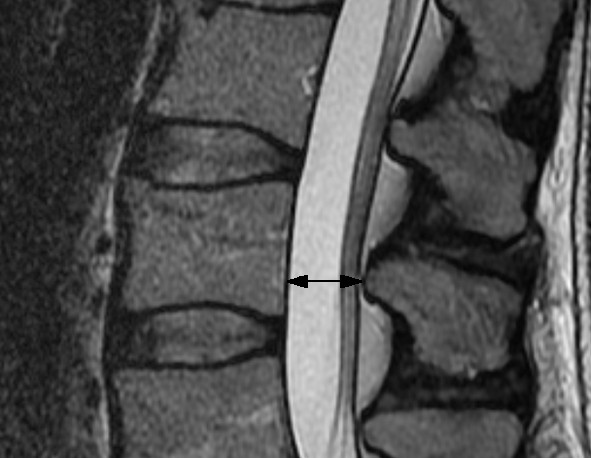
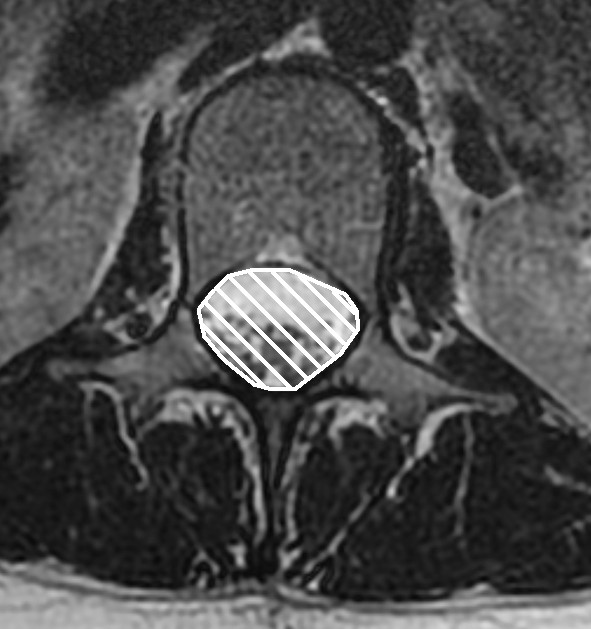
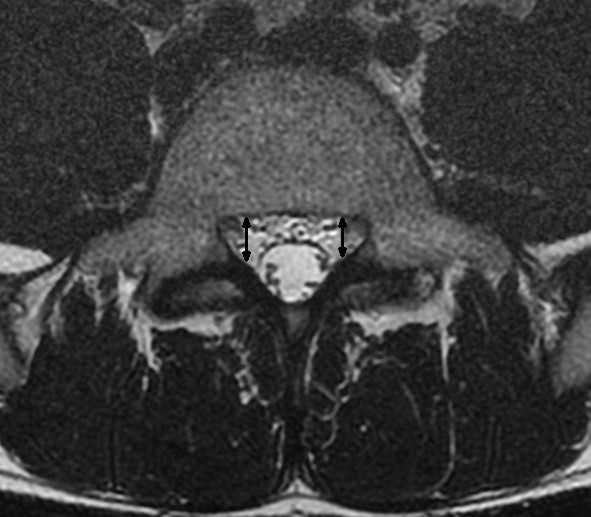
Results: 25 studies reporting on radiological signs of LSS and four systematic reviews related to the evaluation of different treatments were found. Ten different parameters were identified to quantify lumbar spinal stenosis. Most often reported measures for central stenosis were antero-posterior diameter (< 10 mm) and cross-sectional area (< 70 mm(2)) of spinal canal. For lateral stenosis height and depth of the lateral recess, and for foraminal stenosis the foraminal diameter were typically used. Only four of 63 primary studies included in the systematic reviews reported on quantitative measures for defining inclusion criteria of patients in prognostic studies.
Conclusions: There is a need for consensus on well-defined, unambiguous radiological criteria to define lumbar spinal stenosis in order to improve diagnostic accuracy and to formulate reliable inclusion criteria for clinical studies.
Figures



References
-
- North American Spine Society. Evidence Based Clinical Guidelines for Multidisciplinary Spine Care: Diagnosis and Treatment of Degenerative Lumbar Spinal Stenosis. In. Burr Ridge, IL.: North American Spine Society; 2007.
-
- Boden S, Davis D, Dina T, Patronas N, Wiesel S. Abnormal magnetic-resonance scans of the lumbar spine in asymptomatic subjects. A prospective investigation. J Bone Joint Surg Am. 1990;72(3):403–408. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
