

CT imaging features of obturator prostheses in patients following palatectomy or maxillectomy
- PMID: 21799037
- PMCID: PMC7966012
- DOI: 10.3174/ajnr.A2631
CT imaging features of obturator prostheses in patients following palatectomy or maxillectomy
Abstract
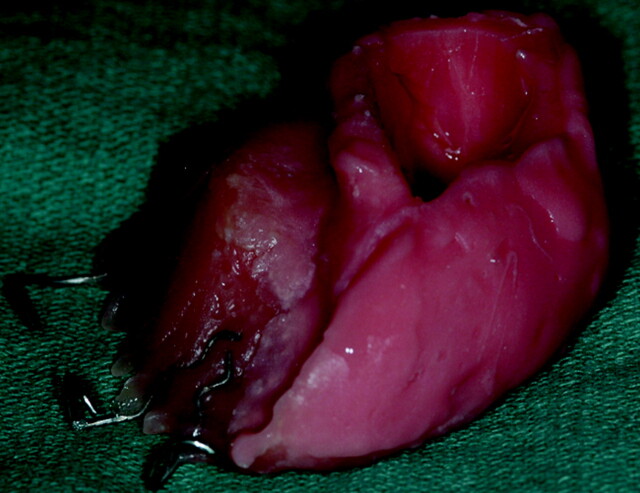
Palatal tumors are often treated with palatectomy or maxillectomy. The resulting surgical defect produces an oroantral communication. An obturator is a removable prosthesis used to close the palatal or maxillectomy defect. Fifteen patients who had undergone palatectomy or maxillectomy for carcinoma and subsequent obturator prosthesis placement were retrospectively studied. Obturators were characterized by Hounsfield units and were subdivided into 3 CT imaging groups: either hyperattenuated, hollow (air-containing), or heterogeneous (isoattenuated to hyperattenuated with internal foci of air). Eight patients had hyperattenuated obturators either representing acrylic resin or Trusoft. Four patients had hollow obturators also composed of acrylic resin or Trusoft. Three patients had heterogeneous obturators, which were composed of only Trusoft. The postoperative imaging of patients treated for palatal or maxillary tumors can be complicated by the presence of obturator prostheses. The intent of this article was to familiarize the reader with the CT imaging features of obturator prostheses.
Figures






References
-
- Ortegon SM, Martin JW, Lewin JS. A hollow delayed surgical obturator for a bilateral subtotal maxillectomy patient: a clinical report. J Prosthet Dent 2008;99:14–18 - PubMed
-
- Keyf F. Obturator prostheses for hemimaxillectomy patients. J Oral Rehabil 2001;28:821–29 - PubMed
-
- Beumer J, III, Curtis TA, Marunick MT. Maxillofacial Rehabilitation: Prosthodontic and Surgical Considerations. St. Louis: Ishiyaku EuroAmerica; 1996:240–85
MeSH terms
LinkOut - more resources
Full Text Sources
Medical