

Obesity and primary graft dysfunction after lung transplantation: the Lung Transplant Outcomes Group Obesity Study
- PMID: 21799077
- PMCID: PMC3208644
- DOI: 10.1164/rccm.201104-0728OC
Obesity and primary graft dysfunction after lung transplantation: the Lung Transplant Outcomes Group Obesity Study
Abstract
Rationale: Obesity has been linked to acute lung injury and is a risk factor for early mortality after lung transplantation.
Objectives: To examine the associations of obesity and plasma adipokines with the risk of primary graft dysfunction after lung transplantation.
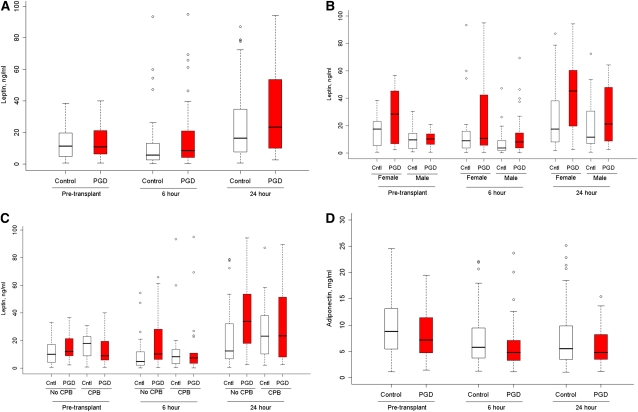
Methods: We performed a prospective cohort study of 512 adult lung transplant recipients with chronic obstructive pulmonary disease or interstitial lung disease enrolled in the Lung Transplant Outcomes Group Study. In a nested case-control study, we measured plasma leptin, adiponectin, and resistin before lung transplantation and 6 and 24 hours after lung transplantation in 40 cases of primary graft dysfunction and 80 control subjects. Generalized linear mixed models and logistic regression were used to estimate risk ratios and odds ratios.
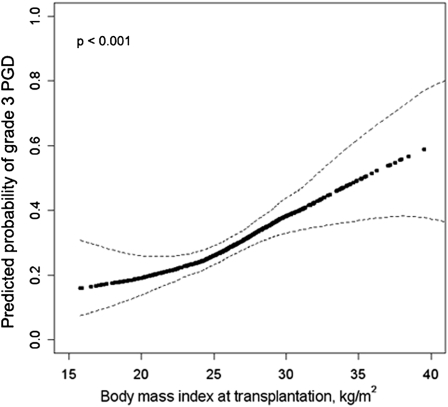
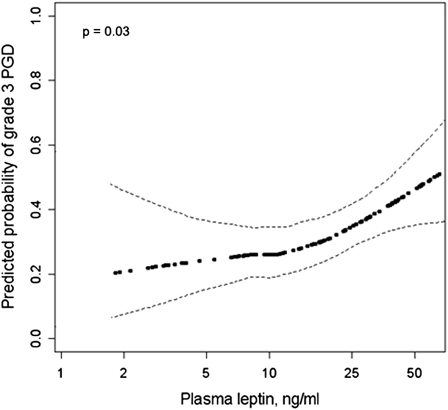
Measurements and main results: Grade 3 primary graft dysfunction developed within 72 hours of transplantation in 29% participants. Obesity was associated with a twofold increased risk of primary graft dysfunction (adjusted risk ratio 2.1; 95% confidence interval, 1.7-2.6). The risk of primary graft dysfunction increased by 40% (confidence interval, 30–50%) for each 5 kg/m(2) increase in body mass index after accounting for center, diagnosis, cardiopulmonary bypass, and transplant procedure. Higher plasma leptin levels were associated with a greater risk of primary graft dysfunction (sex-adjusted P = 0.02). The associations of both obesity and leptin with primary graft dysfunction tended to be stronger among those who did not undergo cardiopulmonary bypass.
Conclusions: Obesity is an independent risk factor for primary graft dysfunction after lung transplantation.
Figures
Comment in
-
Obesity and primary graft dysfunction: weighing the evidence.Am J Respir Crit Care Med. 2011 Nov 1;184(9):994-6. doi: 10.1164/rccm.201108-1431ED. Am J Respir Crit Care Med. 2011. PMID: 22045746 No abstract available.
References
-
- Christie JD, Carby M, Bag R, Corris P, Hertz M, Weill D. Report of the ISHLT working group on primary lung graft dysfunction part II: Definition. A consensus statement of the International Society for Heart and Lung Transplantation. J Heart Lung Transplant 2005;24:1454–1459 - PubMed
-
- Daud SA, Yusen RD, Meyers BF, Chakinala MM, Walter MJ, Aloush AA, Patterson GA, Trulock EP, Hachem RR. Impact of immediate primary lung allograft dysfunction on bronchiolitis obliterans syndrome. Am J Respir Crit Care Med 2007;175:507–513 - PubMed
-
- Whitson BA, Prekker ME, Herrington CS, Whelan TP, Radosevich DM, Hertz MI, Dahlberg PS. Primary graft dysfunction and long-term pulmonary function after lung transplantation. J Heart Lung Transplant 2007;26:1004–1011 - PubMed
-
- de Perrot M, Fischer S, Liu M, Imai Y, Martins S, Sakiyama S, Tabata T, Bai XH, Waddell TK, Davidson BL, et al. Impact of human interleukin-10 on vector-induced inflammation and early graft function in rat lung transplantation. Am J Respir Cell Mol Biol 2003;28:616–625 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
