

Metoprolol impairs resistance artery function in mice
- PMID: 21799135
- PMCID: PMC3774199
- DOI: 10.1152/japplphysiol.01340.2010
Metoprolol impairs resistance artery function in mice
Abstract
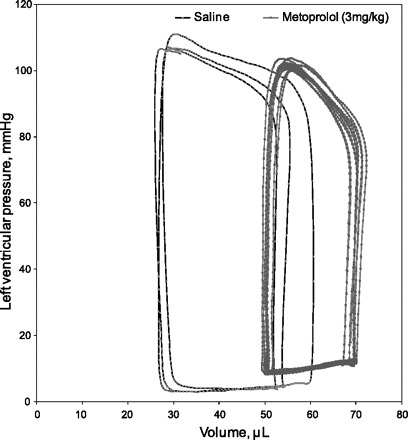
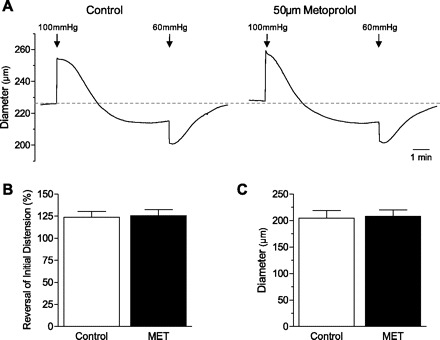
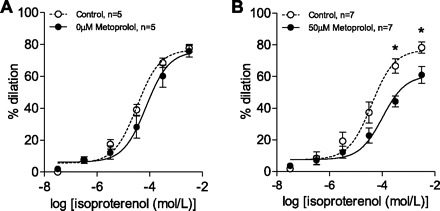
Acute β-blockade with metoprolol has been associated with increased mortality by undefined mechanisms. Since metoprolol is a relatively high affinity blocker of β(2)-adrenoreceptors, we hypothesized that some of the increased mortality associated with its use may be due to its abrogation of β(2)-adrenoreceptor-mediated vasodilation of microvessels in different vascular beds. Cardiac output (CO; pressure volume loops), mean arterial pressure (MAP), relative cerebral blood flow (rCBF; laser Doppler), and microvascular brain tissue Po(2) (G2 oxyphor) were measured in anesthetized mice before and after acute treatment with metoprolol (3 mg/kg iv). The vasodilatory dose responses to β-adrenergic agonists (isoproterenol and clenbuterol), and the myogenic response, were assessed in isolated mesenteric resistance arteries (MRAs; ∼200-μm diameter) and posterior cerebral arteries (PCAs ∼150-μm diameter). Data are presented as means ± SE with statistical significance applied at P < 0.05. Metoprolol treatment did not effect MAP but reduced heart rate and stroke volume, CO, rCBF, and brain microvascular Po(2), while concurrently increasing systemic vascular resistance (P < 0.05 for all). In isolated MRAs, metoprolol did not affect basal artery tone or the myogenic response, but it did cause a dose-dependent impairment of isoproterenol- and clenbuterol-induced vasodilation. In isolated PCAs, metoprolol (50 μM) impaired maximal vasodilation in response to isoproterenol. These data support the hypothesis that acute administration of metoprolol can reduce tissue oxygen delivery by impairing the vasodilatory response to β(2)-adrenergic agonists. This mechanism may contribute to the observed increase in mortality associated with acute administration of metoprolol in perioperative patients.
Figures




References
-
- Anonymous Metoprolol in acute myocardial infarction (MIAMI). A randomised placebo-controlled international trial. The MIAMI Trial Research Group. Eur Heart J 6: 199–226, 1985 - PubMed
-
- Anonymous Randomized.trial of intravenous atenolol among 16 027 cases of suspected acute myocardial infarction: ISIS-1. First International Study of Infarct Survival Collaborative Group. Lancet 2: 57–66, 1986 - PubMed
-
- Badgett RG, Lawrence VA, Cohn SL. Variations in pharmacology of beta-blockers may contribute to heterogeneous results in trials of perioperative beta-blockade. Anesthesiology 113: 585–592, 2010 - PubMed
-
- Bangalore S, Wetterslev J, Pranesh S, Sawhney S, Gluud C, Messerli FH. Perioperative beta blockers in patients having non-cardiac surgery: a meta-analysis. Lancet 372: 1962–1976, 2008 - PubMed
-
- Beattie WS, Karkouti K, Wijeysundera DN, Tait G. Risk associated with preoperative anemia in noncardiac surgery: a single-center cohort study. Anesthesiology 110: 574–581, 2009 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources