

Evaluation of early and late presentation of patients with ocular mucous membrane pemphigoid to two major tertiary referral hospitals in the United Kingdom
- PMID: 21799523
- PMCID: PMC3173873
- DOI: 10.1038/eye.2011.175
Evaluation of early and late presentation of patients with ocular mucous membrane pemphigoid to two major tertiary referral hospitals in the United Kingdom
Abstract
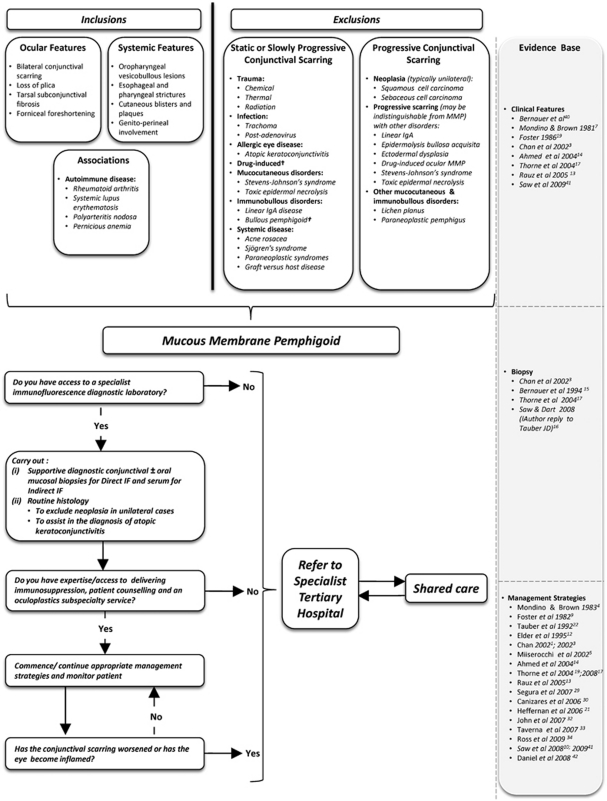
Purpose: Ocular mucous membrane pemphigoid (OcMMP) is a sight-threatening autoimmune disease in which referral to specialists units for further management is a common practise. This study aims to describe referral patterns, disease phenotype and management strategies in patients who present with either early or established disease to two large tertiary care hospitals in the United Kingdom.
Patients and methods: In all, 54 consecutive patients with a documented history of OcMMP were followed for 24 months. Two groups were defined: (i) early-onset disease (EOD:<3 years, n=26, 51 eyes) and (ii) established disease (EstD:>5 years, n=24, 48 eyes). Data were captured at first clinic visit, and at 12 and 24 months follow-up. Information regarding duration, activity and stage of disease, visual acuity (VA), therapeutic strategies and clinical outcome were analysed.
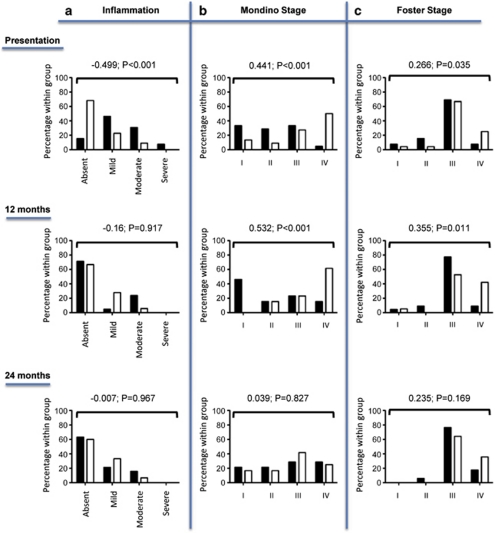
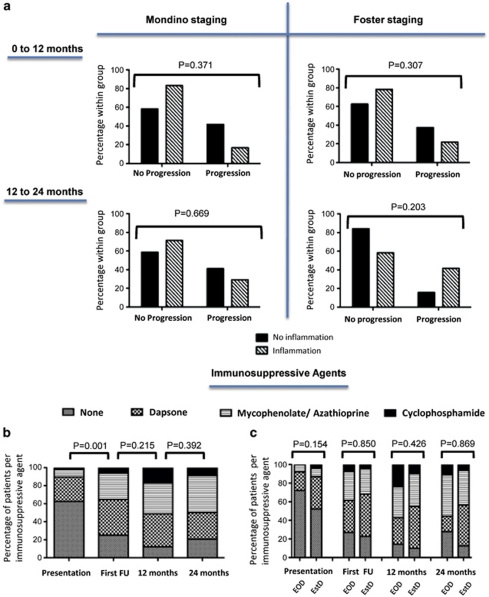
Results: Patients with EOD were younger and had more severe conjunctival inflammation (76% of inflamed eyes) than the EstD group, who had poorer VA (26.7%=VA<3/60, P<0.01) and more advanced disease. Although 40% of patients were on existing immunosuppression, 48% required initiation or switch to more potent immunotherapy. In all, 28% (14) were referred back to the originating hospitals for continued care. Although inflammation had resolved in 78% (60/77) at 12 months, persistence of inflammation and progression did not differ between the two phenotypes. Importantly, 42% demonstrated disease progression in the absence of clinically detectable inflammation.
Conclusions: These data highlight that irrespective of OcMMP phenotype, initiation or escalation of potent immunosuppression is required at tertiary hospitals. Moreover, the conjunctival scarring progresses even when the eye remains clinically quiescent. Early referral to tertiary centres is recommended to optimise immunosuppression and limit long-term ocular damage.
Figures
Comment in
-
The evil curse of ocular pemphigoid.Eye (Lond). 2011 Sep;25(9):1107-8. doi: 10.1038/eye.2011.181. Eye (Lond). 2011. PMID: 21900957 Free PMC article. No abstract available.
References
-
- Chan LS. Mucous membrane pemphigoid. Clin Dermatol. 2001;19:703–711. - PubMed
-
- Risser J, Lewis K, Weinstock MA. Mortality of bullous skin disorders from 1979 through 2002 in the United States. Arch Dermatol. 2009;145 (9:1005–1008. - PubMed
-
- Chan LS, Ahmed AR, Anhalt GJ, Bernauer W, Cooper KD, Elder MJ, et al. The first international consensus on mucous membrane pemphigoid: definition, diagnostic criteria, pathogenic factors, medical treatment, and prognostic indicators. Arch Dermatol. 2002;138:370–379. - PubMed
-
- Mondino BJ, Brown SI. Immunosuppressive therapy in ocular cicatricial pemphigoid. Am J Ophthalmol. 1983;96:453–459. - PubMed
-
- Miserocchi E, Baltatzis S, Roque MR, Ahmed AR, Foster CS. The effect of treatment and its related side effects in patients with severe ocular cicatricial pemphigoid. Ophthalmology. 2002;109:111–118. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
