

Outcomes of multi-drug resistant tuberculosis (MDR-TB) among a cohort of South African patients with high HIV prevalence
- PMID: 21799728
- PMCID: PMC3142109
- DOI: 10.1371/journal.pone.0020436
Outcomes of multi-drug resistant tuberculosis (MDR-TB) among a cohort of South African patients with high HIV prevalence
Abstract
Background: Multidrug-resistant tuberculosis (MDR-TB) is a major clinical challenge, particularly in patients with human immunodeficiency virus (HIV) co-infection. MDR-TB treatment is increasingly available, but outcomes have not been well characterized. South Africa has provided MDR-TB treatment for a decade, and we evaluated outcomes by HIV status for patients enrolled between 2000 and 2004 prior to anti-retroviral access.
Methods: We assessed treatment outcomes in a prospective cohort of patients with MDR-TB from eight provincial programs providing second line drugs. World Health Organization definitions were used. Results were stratified by HIV status.
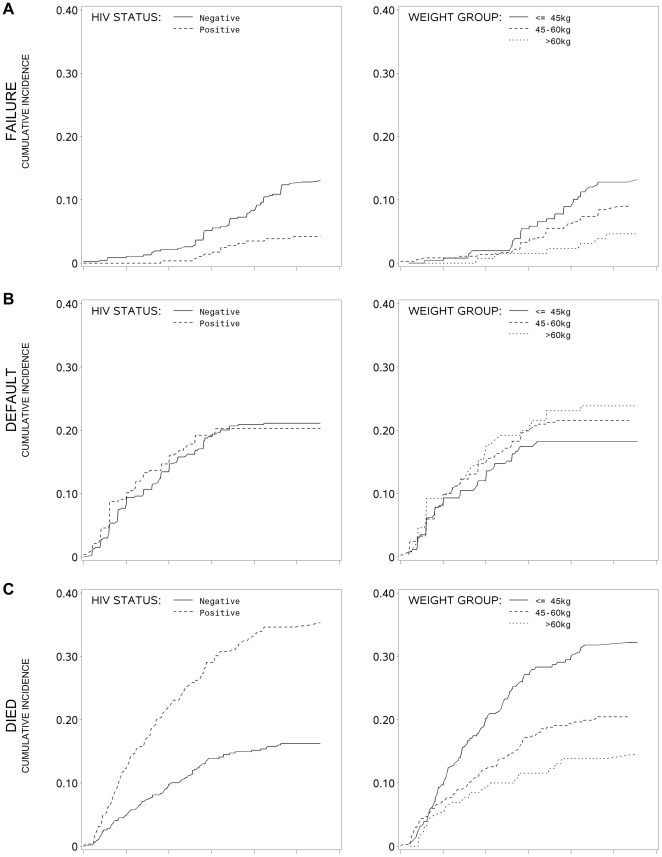
Results: Seven hundred fifty seven patients with known HIV status were included in the final analysis, and HIV infection was documented in 287 (38%). Overall, 348 patients (46.0%) were successfully treated, 74 (9.8%) failed therapy, 177 (23.4%) died and 158 (20.9%) defaulted. Patients with HIV were slightly younger and less likely to be male compared to HIV negative patients. Patients with HIV were less likely to have a successful treatment outcome (40.0 vs. 49.6; P<0.05) and more likely to die (35.2 vs. 16.2; P<0.0001). In a competing risk survival analysis, patients with HIV had a higher hazard of death (HR: 2.33, P<0.0001). Low baseline weight (less than 45 kg and less than 60 kg) was also associated with a higher hazard of death (HR: 2.52, P<0.0001; and HR: 1.50, P<0.0001, respectively, compared to weight greater than 60 kg). Weight less than 45 kg had higher risk of failure (HR: 3.58, P<0.01). Any change in treatment regimen was associated with a higher hazard of default (HR: 2.86; 95% CI 1.55-5.29, P<0.001) and a lower hazard of death (HR: 0.63, P<0.05).
Conclusions: In this MDR-TB treatment program patients with HIV infection and low weight had higher hazards of death. Overall treatment outcomes were poor. Efforts to improve treatment for MDR-TB are urgently needed.
Conflict of interest statement
Figures
References
-
- Ahmad S, Al-Mutairi NM, Mokaddas E. Comparison of performance of two DNA line probe assays for rapid detection of multidrug-resistant isolates of Mycobacterium tuberculosis. Indian J Exp Biol. 2009;47:454–462. - PubMed
-
- Shah NS, Moodley P, Babaria P, Moodley S, Ramtahal M, et al. Rapid diagnosis of tuberculosis and multidrug resistance by the microscopic-observation drug-susceptibility assay. Am J Respir Crit Care Med. 2011;183:1427–1433. - PubMed
-
- World Health Organization. Geneva, Switzerland: 2010. Multidrug and extensively drug-resistant TB (M/XDR-TB): 2010 Global Report on Surveillance and Response.
-
- World Health Organization. Geneva: 2008. Tuberculosis MDR-TB & XDR-TB: The 2008 Report.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
