

The impact of the new WHO antiretroviral treatment guidelines on HIV epidemic dynamics and cost in South Africa
- PMID: 21799755
- PMCID: PMC3140490
- DOI: 10.1371/journal.pone.0021919
The impact of the new WHO antiretroviral treatment guidelines on HIV epidemic dynamics and cost in South Africa
Abstract
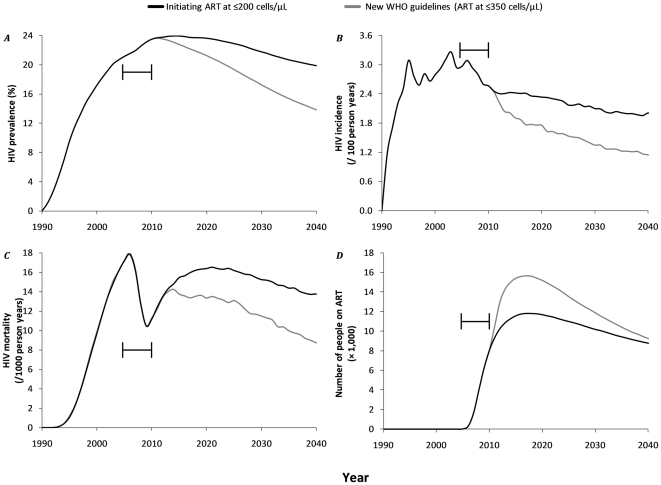
Background: Since November 2009, WHO recommends that adults infected with HIV should initiate antiretroviral therapy (ART) at CD4+ cell counts of ≤350 cells/µl rather than ≤200 cells/µl. South Africa decided to adopt this strategy for pregnant and TB co-infected patients only. We estimated the impact of fully adopting the new WHO guidelines on HIV epidemic dynamics and associated costs.
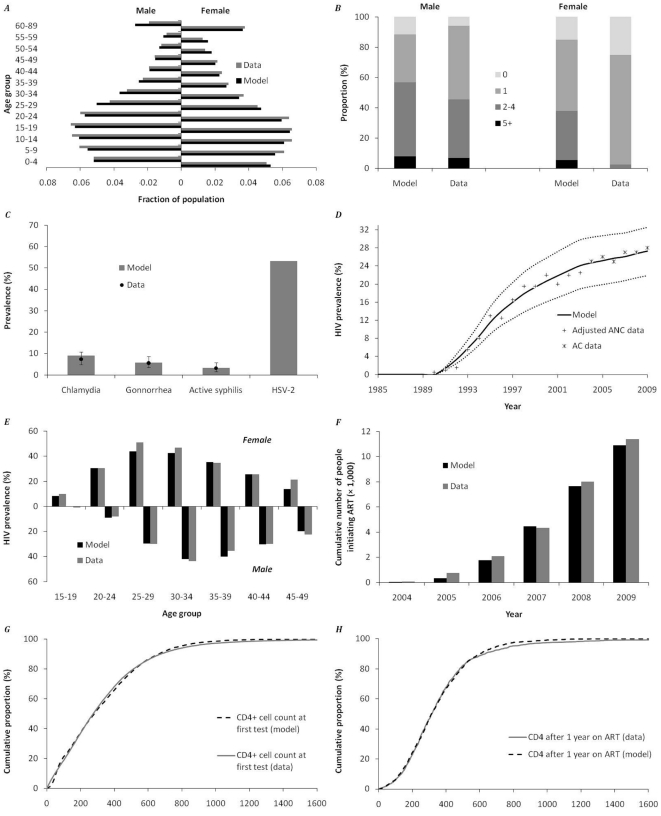
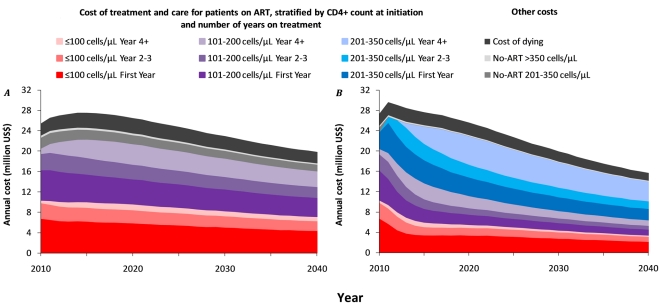
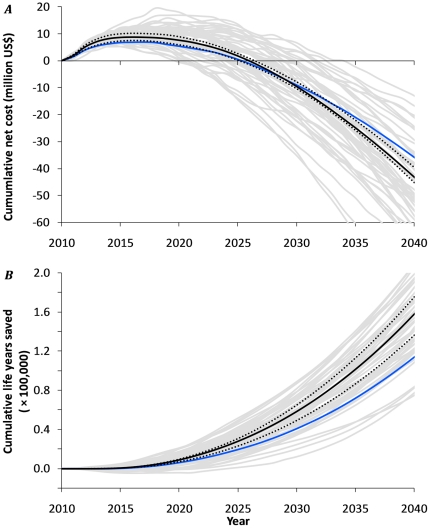
Methods and finding: We used an established model of the transmission and control of HIV in specified sexual networks and healthcare settings. We quantified the model to represent Hlabisa subdistrict, KwaZulu-Natal, South Africa. We predicted the HIV epidemic dynamics, number on ART and program costs under the new guidelines relative to treating patients at ≤200 cells/µl for the next 30 years. During the first five years, the new WHO treatment guidelines require about 7% extra annual investments, whereas 28% more patients receive treatment. Furthermore, there will be a more profound impact on HIV incidence, leading to relatively less annual costs after seven years. The resulting cumulative net costs reach a break-even point after on average 16 years.
Conclusions: Our study strengthens the WHO recommendation of starting ART at ≤350 cells/µl for all HIV-infected patients. Apart from the benefits associated with many life-years saved, a modest frontloading appears to lead to net savings within a limited time-horizon. This finding is robust to alternative assumptions and foreseeable changes in ART prices and effectiveness. Therefore, South Africa should aim at rapidly expanding its healthcare infrastructure to fully embrace the new WHO guidelines.
Conflict of interest statement
Figures
References
-
- WHO. Rapid Advice: Antiretroviral therapy for HIV infected adults and adolescents. Geneva: World Health Organization. 2009 Available: www.who.int/hiv/pub/arv/rapid_advice_art.pdf Accessed 2011 Jan 30.
-
- SANAC. The South African antiretroviral treatment guidelines 2010. Pretoria: South African National AIDS Council. 2010 Available: http://www.sanac.org.za/resources/art-guidelines. Accessed 2010 Dec 20.
-
- SANAC. Media statement: outline of the national HIV counseling and testing (HTC) campaign. 2010 Available: http://www.sanac.org.za/documents/Media%20Statement%2025%2003%2010.pdf. Accessed 2010 Apr 30.
-
- Palella FJ, Jr, Delaney KM, Moorman AC, Loveless MO, Furher J, et al. Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. N Eng J Med. 1998;338:853–860. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
