

Measuring enzymatic HIV-1 susceptibility to two reverse transcriptase inhibitors as a rapid and simple approach to HIV-1 drug-resistance testing
- PMID: 21799767
- PMCID: PMC3140485
- DOI: 10.1371/journal.pone.0022019
Measuring enzymatic HIV-1 susceptibility to two reverse transcriptase inhibitors as a rapid and simple approach to HIV-1 drug-resistance testing
Abstract
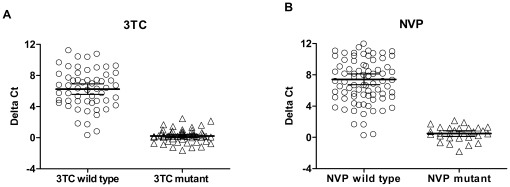
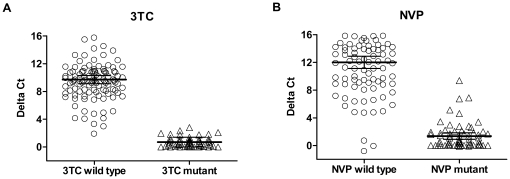
Simple and cost-effective approaches for HIV drug-resistance testing are highly desirable for managing increasingly expanding HIV-1 infected populations who initiate antiretroviral therapy (ART), particularly in resource-limited settings. Non-nucleoside reverse trancriptase inhibitor (NNRTI)-based regimens with an NRTI backbone containing lamivudine (3TC) or emtricitabine (FTC) are preferred first ART regimens. Failure with these drug combinations typically involves the selection of NNRTI- and/or 3TC/FTC-resistant viruses. Therefore, the availability of simple assays to measure both types of drug resistance is critical. We have developed a high throughput screening test for assessing enzymatic resistance of the HIV-1 RT in plasma to 3TC/FTC and NNRTIs. The test uses the sensitive "Amp-RT" assay with a newly-developed real-time PCR format to screen biochemically for drug resistance in single reactions containing either 3TC-triphosphate (3TC-TP) or nevirapine (NVP). Assay cut-offs were defined based on testing a large panel of subtype B and non-subtype B clinical samples with known genotypic profiles. Enzymatic 3TC resistance correlated well with the presence of M184I/V, and reduced NVP susceptibility was strongly associated with the presence of K103N, Y181C/I, Y188L, and G190A/Q. The sensitivity and specificity for detecting resistance were 97.0% and 96.0% in samples with M184V, and 97.4% and 96.2% for samples with NNRTI mutations, respectively. We further demonstrate the utility of an HIV capture method in plasma by using magnetic beads coated with CD44 antibody that eliminates the need for ultracentifugation. Thus our results support the use of this simple approach for distinguishing WT from NNRTI- or 3TC/FTC-resistant viruses in clinical samples. This enzymatic testing is subtype-independent and can assist in the clinical management of diverse populations particularly in resource-limited settings.
Conflict of interest statement
Figures
References
-
- Richman DD. HIV chemotherapy. Nature. 2001;410:995–1001. - PubMed
-
- Deeks SG. Treatment of antiretroviral-drug-resistant HIV-1 infection. Lancet. 2003;362:2002–11. - PubMed
-
- Johnson VA, Brun-Vezinet F, Clotet B, Gunthard HF, Kuritzkes DR, et al. Update of the drug resistance mutations in HIV-1: December 2009. Top HIV Med. 2009;17:138–45. - PubMed
-
- EuroGuidelines Group for HIV Resistance. Clinical and laboratory guidelines for the use of HIV-1 drug resistance testing as part of treatment management: recommendations for the European setting. The EuroGUidelines Group for HIV resistance. Aids. 2001;15:309–20. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
