

Shifting trends in liver-directed management of patients with colorectal liver metastasis: a population-based analysis
- PMID: 21801959
- PMCID: PMC3568532
- DOI: 10.1016/j.surg.2011.06.013
Shifting trends in liver-directed management of patients with colorectal liver metastasis: a population-based analysis
Abstract
Background: We sought to evaluate population-based temporal trends in perioperative management, as well as short- and long-term outcomes associated with the operative management of colorectal liver metastasis (CRLM).
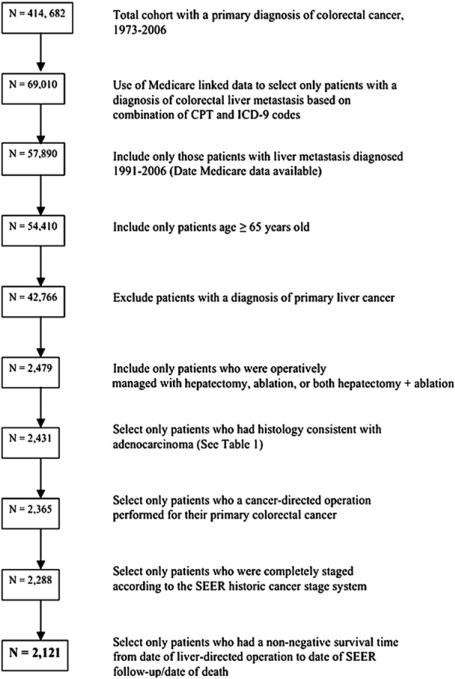
Methods: Using Surveillance, Epidemiology and End Results-Medicare linked data, we identified 2,121 patients with operatively managed CRLM between 1991 and 2006. Clinicopathologic data, trends in operative management, and survival were examined.
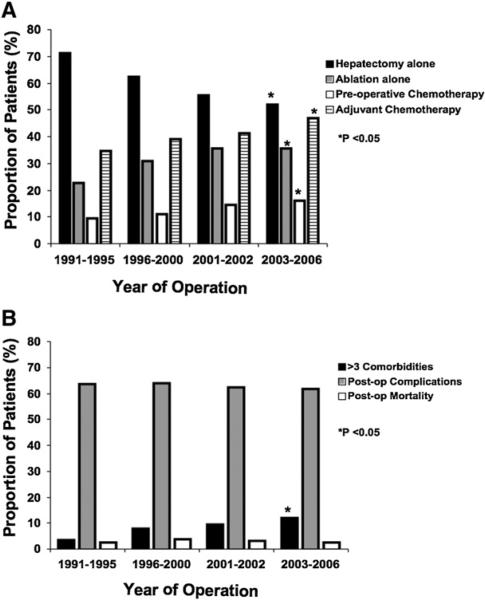
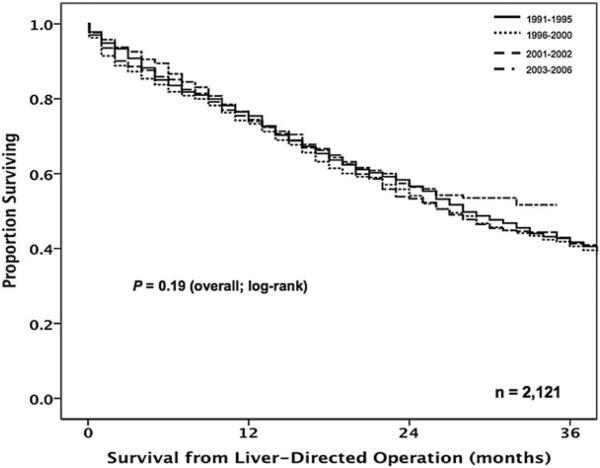
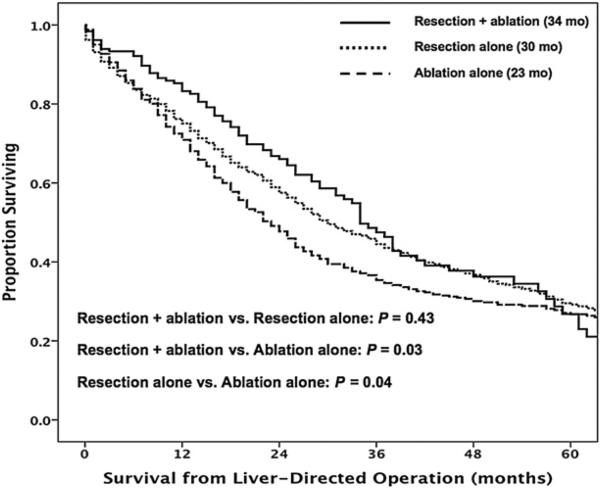
Results: Preoperative evaluation included computed tomography (CT; 66%), magnetic resonance imaging (MRI; 5%), and positron emission tomography (PET; 2%) with a temporal increase in the use of all 3 modalities over time (all P < .05). Patients undergoing hepatectomy only (n = 1,267; 60%) decreased over time, whereas the use of ablation alone (n = 668; 32%) and combined resection plus ablation (n = 186; 9%) increased (all P < .05). The use of both preoperative (10% to 16%) and adjuvant chemotherapy (35% to 47%) increased over time (P < .05). There was a marked temporal increase in patient comorbidities (>3 comorbidities: 1991-1995, 3%; 2003-2006, 12%; P < .001); however, perioperative complications (63%) and 30-day mortality (3%) did not change over time (both P > .05); 90-day mortality decreased from 9% to 7% over the study period (P = .007). Overall the 1-, 3-, and 5-year survivals were 74%, 42%, and 28% with no improvement over time (P = .19). On multivariate analysis, synchronous disease (hazard ratio [HR], 1.7) and use of ablation alone (HR, 1.2) were associated independently with a worse survival (both P < .05).
Conclusion: Most patients were evaluated with CT; PET was employed rarely. Although there was a temporal increase in chemotherapy utilization, only one half of patients received perioperative chemotherapy. Mortality associated with hepatic operations was low, but morbidity remained high with no temporal change despite an increased number of patient medical comorbidities.
Copyright © 2011 Mosby, Inc. All rights reserved.
Figures
References
-
- Jemal A, Siegel R, Ward E, Hao Y, Xu J, Thun MJ. Cancer Statistics, 2009. CA Cancer J Clin. 2009;59:225–49. - PubMed
-
- Norstein J, Silen W. Natural history of liver metastases from colorectal carcinoma. J Gastrointest Surg. 1997;1:398–407. - PubMed
-
- Blumgart LH, Allison DJ. Resection and embolization in the management of secondary hepatic tumors. World J Surg. 1982;6:32–45. - PubMed
-
- Taylor I, Mullee MA, Campbell MJ. Prognostic index for the development of liver metastases in patients with colorectal cancer. Br J Surg. 1990;77:499–501. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
