

TMPRSS2-ERG status in circulating tumor cells as a predictive biomarker of sensitivity in castration-resistant prostate cancer patients treated with abiraterone acetate
- PMID: 21802835
- PMCID: PMC3185163
- DOI: 10.1016/j.eururo.2011.07.011
TMPRSS2-ERG status in circulating tumor cells as a predictive biomarker of sensitivity in castration-resistant prostate cancer patients treated with abiraterone acetate
Abstract
Background: Abiraterone acetate (AA) is an androgen biosynthesis inhibitor shown to prolong life in patients with castration-resistant prostate cancer (CRPC) already treated with chemotherapy. AA treatment results in dramatic declines in prostate-specific antigen (PSA) in some patients and no declines in others, suggesting the presence of molecular determinants of sensitivity in tumors.
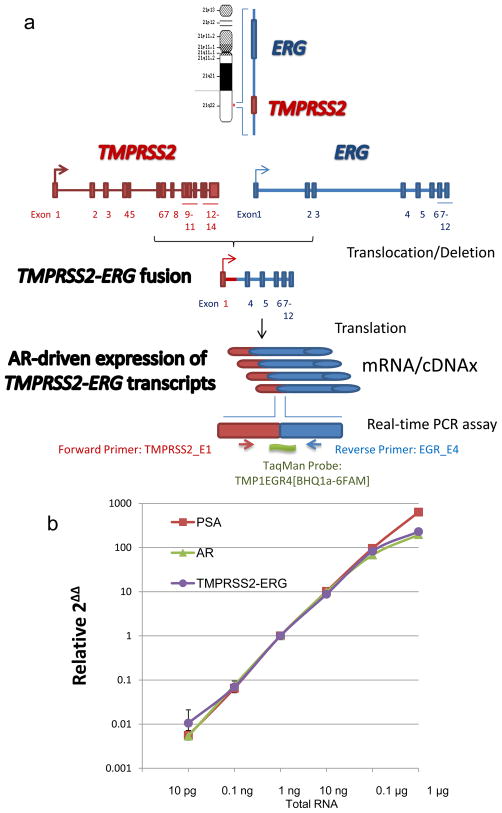
Objective: To study the role of transmembrane protease, serine 2 (TMPRSS2)-v-ets erythroblastosis virus E26 oncogene homolog (ERG) fusion, an androgen-dependent growth factor, in circulating tumor cells (CTCs) as a biomarker of sensitivity to AA.
Design, setting, and participants: The predictive value of TMPRSS2-ERG status was studied in 41 of 48 men with postchemotherapy-treated CRPC enrolled in sequential phase 2 AA trials.
Intervention: Patients received AA 1000 mg daily and continuously.
Measurements: TMPRSS2-ERG status was characterized by a sensitive, analytically valid reverse transcription polymerase chain reaction assay in CTCs enriched from ethylene-diaminetetraacetic acid anticoagulated blood obtained prior to AA treatment. Outcomes were measured by PSA Working Group 1 criteria.
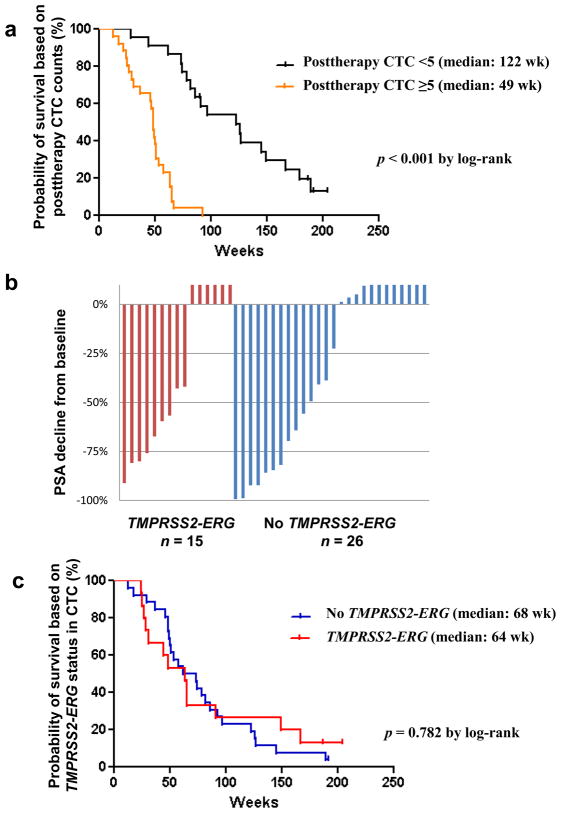
Results and limitations: Standard procedures for specimen acquisition, processing, and testing using the validated TMPRSS2-ERG assay on a multiplex platform gave intra-assay and interassay coefficients of variation <7%. TMPRSS2-ERG fusion was present in 15 of 41 patients (37%), who had a median baseline CTC count of 17 (interquartile range: 7-103 cells per 7.5 ml). A PSA decline ≥50% was observed in 7 of 15 patients (47%) with the fusion and in 10 of 26 patients (38%) without the fusion. Although limited by the low number of patients, a posttherapy CTC count of less than five per 7.5 ml was prognostic for longer survival relative to a CTC count five or more. TMPRSS2-ERG status did not predict a decline in PSA or other clinical outcomes.
Conclusions: Molecular profiles of CTCs with an analytically valid assay identified the presence of the prostate cancer-specific TMPRSS2-ERG fusion but did not predict for response to AA treatment. This finding demonstrates the role of CTCs as surrogate tissue that can be obtained in a routine practice setting.
Trial registration: ClinicalTrials.gov: NCT00474383 (COU-AA-003), NCT00485303 (COU-AA-004).
Copyright © 2011 European Association of Urology. Published by Elsevier B.V. All rights reserved.
Figures
Comment in
-
Circulating tumour cells as surrogate biomarkers in castration-resistant prostate cancer trials.Eur Urol. 2011 Nov;60(5):905-7. doi: 10.1016/j.eururo.2011.08.024. Epub 2011 Aug 19. Eur Urol. 2011. PMID: 21871707 No abstract available.
References
-
- Scher HI, Sawyers C. Biology of progressive castration resistant prostate cancer: directed therapies targeting the androgen receptor signaling axis. J Clin Oncol. 2005;23:8253–61. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
