

Prior failed ipsilateral percutaneous endovascular intervention in patients with critical limb ischemia predicts poor outcome after lower extremity bypass
- PMID: 21802888
- PMCID: PMC5292259
- DOI: 10.1016/j.jvs.2011.03.236
Prior failed ipsilateral percutaneous endovascular intervention in patients with critical limb ischemia predicts poor outcome after lower extremity bypass
Abstract
Background: Although open surgical bypass remains the standard revascularization strategy for patients with critical limb ischemia (CLI), many centers now perform peripheral endovascular intervention (PVI) as the first-line treatment for these patients. We sought to determine the effect of a prior ipsilateral PVI (iPVI) on the outcome of subsequent lower extremity bypass (LEB) in patients with CLI.
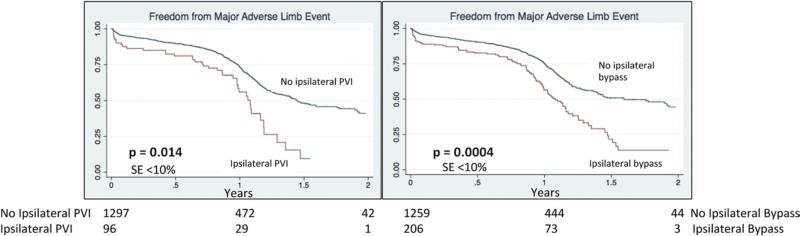
Methods: A retrospective cohort analysis of all patients undergoing infrainguinal LEB between 2003 and 2009 within hospitals comprising the Vascular Study Group of New England (VSGNE) was performed. Primary study endpoints were major amputation and graft occlusion at 1 year postoperatively. Secondary outcomes included in-hospital major adverse events (MAE), 1-year mortality, and composite 1-year major adverse limb events (MALE). Event rates were determined using life table analyses and comparisons were performed using the log-rank test. Multivariate predictors were determined using a Cox proportional hazards model with multilevel hierarchical adjustment.
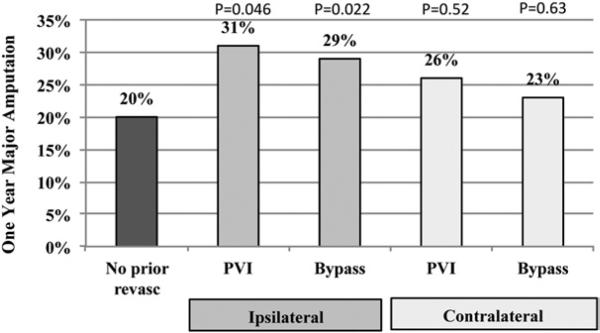
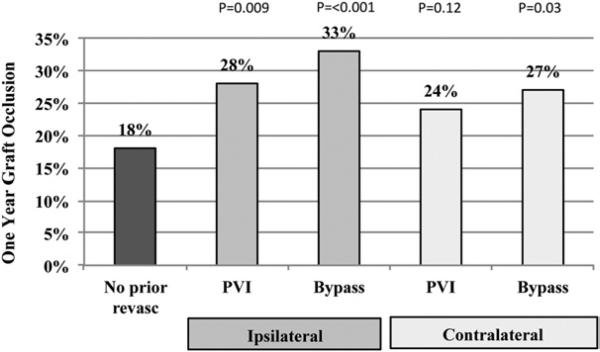
Results: Of 1880 LEBs performed, 32% (n = 603) had a prior infrainguinal revascularization procedure (iPVI, 7%; ipsilateral bypass, 15%; contralateral PVI, 3%; contralateral bypass, 17%). Patients with prior iPVI, compared with those without a prior iPVI, were more likely to be women (32 vs 41%; P = .04), less likely to have tissue loss (52% vs 63%; P = .02), more likely to require arm vein conduit (16% vs 5%; P = .001), and more likely to be on statin (71% vs 54%; P = .01) and beta blocker therapy (92% vs 81%; P = .01) at the time of their bypass procedure. Other demographic factors were similar between these groups. Prior PVI or bypass did not alter 30-day MAE and 1-year mortality after the index bypass. In contrast, 1-year major amputation and 1-year graft occlusion rates were significantly higher in patients who had prior iPVI than those without (31% vs 20%; P = .046 and 28% vs 18%; P = .009), similar to patients who had a prior ipsilateral bypass (1 year major amputation, 29% vs 20%; P = .022; 1 year graft occlusion, 33% vs 18%; P = .001). Independent multivariate predictors of higher 1-year amputation and graft occlusion rates were prior iPVI, prior ipsilateral bypass, dialysis dependence, prosthetic conduit and distal (tibial and pedal) bypass target.
Conclusions: Prior iPVI is highly predictive for poor outcome in patients undergoing LEB for CLI with higher 1-year amputation and graft occlusion rates than those without prior revascularization, similar to prior ipsilateral bypass These findings provide information, which may help with the complex decisions surrounding revascularization options in patients with CLI.
Copyright © 2011 Society for Vascular Surgery. Published by Mosby, Inc. All rights reserved.
Figures
References
-
- Varu VN, Hogg ME, Kibbe MR. Critical limb ischemia. J Vasc Surg. 2010;51:230–41. - PubMed
-
- Bradbury AW, Adam DJ, Bell J, Forbes JF, Fowkes FG, Gillespie I, et al. Bypass versus Angioplasty in Severe Ischaemia of the Leg (BASIL) trial: an intention-to-treat analysis of amputation-free and overall survival in patients randomized to a bypass surgery-first or a balloon angioplastyfirst revascularization strategy. J Vasc Surg. 2010;51:5S–17S. - PubMed
-
- Bradbury AW, Adam DJ, Bell J, Forbes JF, Fowkes FG, Gillespie I, et al. Bypass versus angioplasty in severe ischaemia of the leg (BASIL) trial: analysis of amputation free and overall survival by treatment received. J Vasc Surg. 2010;51:18S–31S. - PubMed
-
- Böckler D, Blaurock P, Mansmann U, Schwarzbach M, Seelos R, Schumacher H, et al. Early surgical outcome after failed primary stenting for lower limb occlusive disease. J Endovasc Ther. 2005;12:13–21. - PubMed
-
- Joels CS, York JW, Kalbaugh CA, Cull DL, Langan EM III, Taylor SM, et al. Surgical implications of early failed endovascular intervention of the superficial femoral artery. J Vasc Surg. 2008;47:562–5. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
