

doi: 10.1016/j.ccl.2011.06.002.
Exercise intolerance
Affiliations
- PMID: 21803233
- PMCID: PMC3694583
- DOI: 10.1016/j.ccl.2011.06.002
Item in Clipboard
Exercise intolerance
Cardiol Clin.
2011 Aug.
Abstract
Exercise intolerance is the primary symptom of chronic diastolic heart failure. It is part of the definition of heart failure and is intimately linked to its pathophysiology. Further, exercise intolerance affects the diagnosis and prognosis of heart failure. In addition, understanding the mechanisms of exercise intolerance can lead to developing and testing rational treatments for heart failure. This article focuses on the fundamental principles of exercise physiology and on the assessment, pathophysiology, and potential treatment of exercise intolerance in diastolic heart failure.
Copyright © 2011 Elsevier Inc. All rights reserved.
Figures
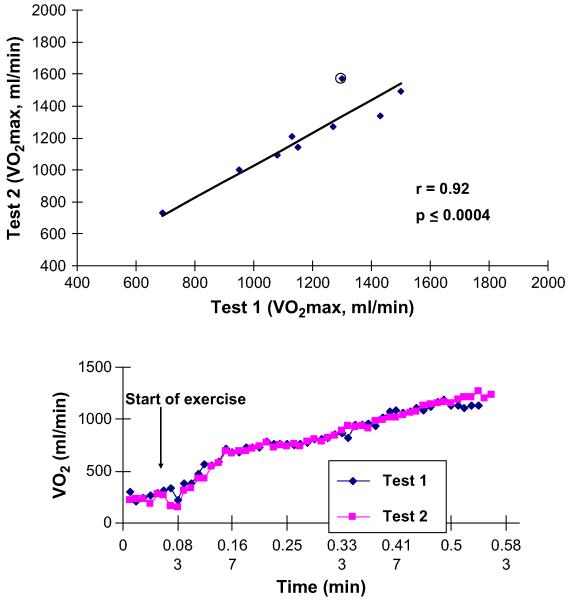
Excellent reproducibility of peak exercise VO2 in older patients who have heart failure, including those who have LVEF. (Top panel) Group data. (Bottom panel) 15-Second averaged data from a representative patient. (From Marburger CT, Brubaker PH, Pollock WE, et al. Reproducibility of cardiopulmonary exercise testing in elderly heart failure patients. Am J Cardiol 1998;82:905-9; with permission.)
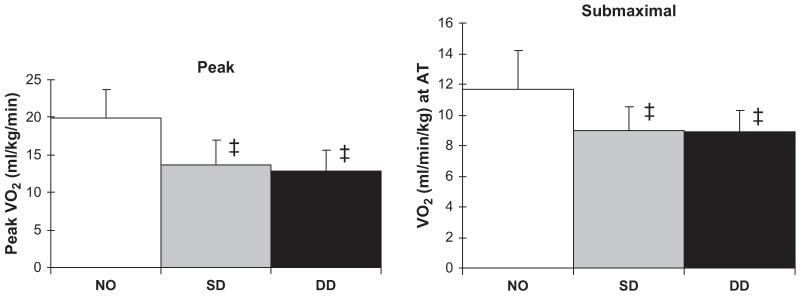
VO2 during peak exhaustive exercise (left panel) and during submaximal exercise at the ventilatory anaerobic threshold (right panel) in age-matched normal subjects (NO), elderly patients who have heart failure caused by systolic dysfunction (SD), and elderly patients who have heart failure with normal systolic function, that is, presumed diastolic dysfunction (DD). Exercise capacity is severely reduced in patients who have DHF compared with normal controls (P<.001), to a degree similar to the reduction in patients who have SHF. Overall, peak exercise VO2 was 33% lower in the women than in the men (not shown). (Data from Kitzman DW, Little WC, Brubaker PH, et al. Pathophysiological characterization of isolated diastolic heart failure in comparison to systolic heart failure. JAMA 2002;288(17):2144-50.)
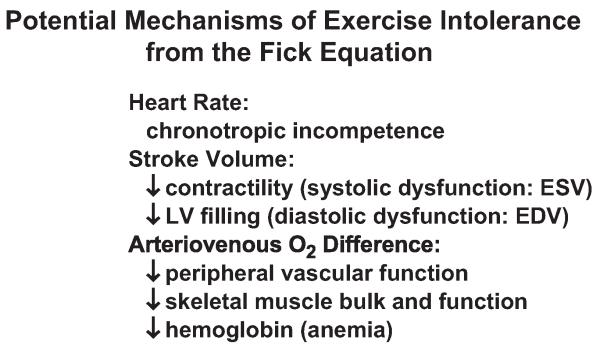
Potential mechanisms of exercise intolerance from the factors of the Fick equation. EDV, enddiastolic volume; ESV, end-systolic volume.
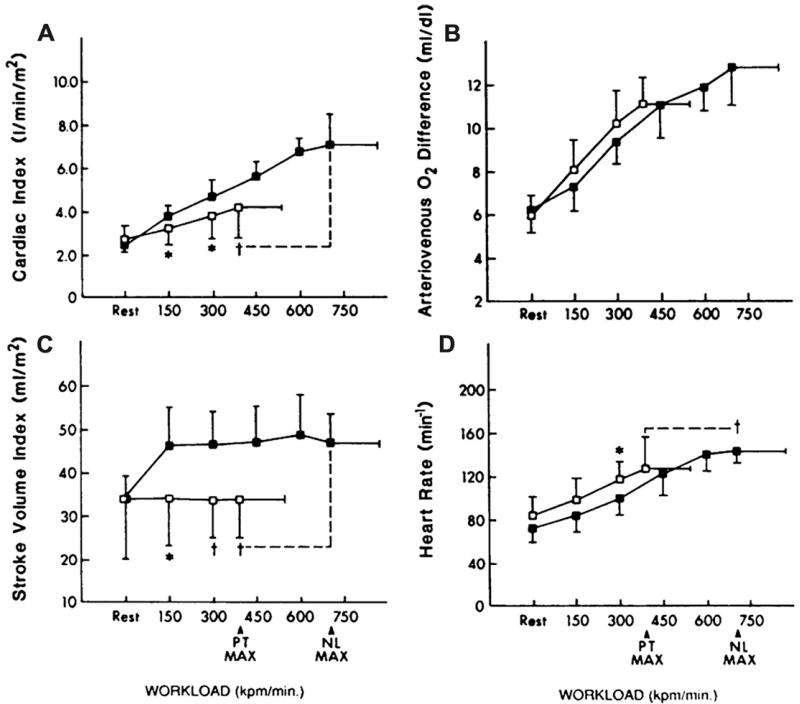
Cardiovascular function assessed by invasive cardiopulmonary exercise testing in patients who have heart failure and normal systolic function (open boxes) and age-matched normal controls (closed boxes). The primary components of the Fick equation for VO2, cardiac output, and A-VO2 difference are shown in panels A and B, respectively. The components of cardiac output, stroke volume, and heart rate are shown in panels C and D. The X-axis is exercise workload in kilopounds/min (kpm); 150 kpm is equivalent to 25 W. (From Kitzman DW, Higginbotham MB, Cobb FR, et al. Exercise intolerance in patients with heart failure and preserved left ventricular systolic function: failure of the Frank-Starling mechanism. J Am Coll Cardiol 1991;17:1065-72; with permission. Copyright © 1991, American College of Cardiology.)
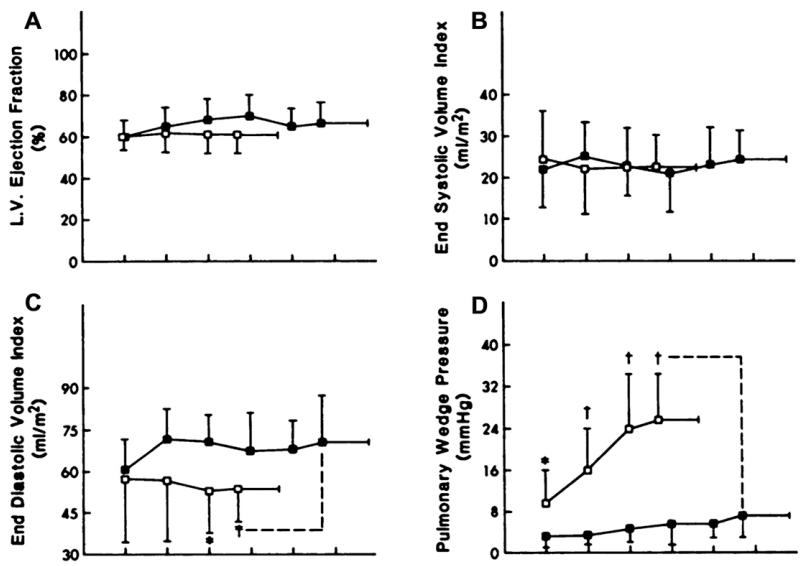
The components of the LV stroke volume response during exercise, LVEF, end-systolic volume, end-diastolic volume, and LV filling pressure are shown in panels A-D. Not shown are systolic and mean arterial pressures, which were not different between groups. The key is the same as in Fig. 4. (From Kitzman DW, Higginbotham MB, Cobb FR, et al. Exercise intolerance in patients with heart failure and preserved left ventricular systolic function: failure of the Frank-Starling mechanism. J Am Coll Cardiol 1991;17:1065-72; with permission. Copyright © 1991, American College of Cardiology.)
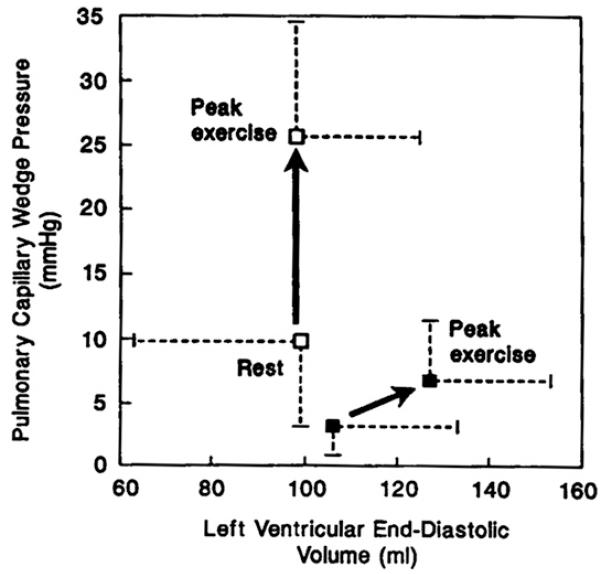
LV diastolic function assessed by invasive cardiopulmonary exercise testing. The key is the same as in Fig. 4. The pressure-volume relationship was shifted upward and leftward at rest. In the patients undergoing exercise testing, LV diastolic volume did not increase despite the marked increase in diastolic (pulmonary wedge) pressure. Because of diastolic dysfunction, failure of the Frank-Starling mechanism resulted in severe exercise intolerance. (From Kitzman DW, Higginbotham MB, Cobb FR, et al. Exercise intolerance in patients with heart failure and preserved left ventricular systolic function: failure of the Frank-Starling mechanism. J Am Coll Cardiol 1991;17:1065-72; with permission. Copyright © 1991, American College of Cardiology.)
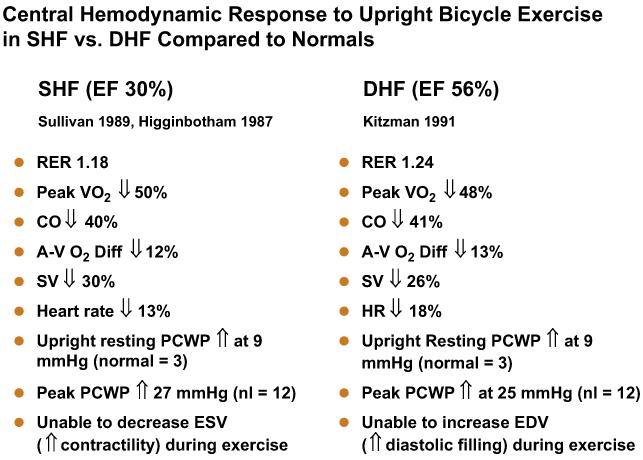
Comparison of characteristic central and peripheral cardiovascular response to exercise in patients who have heart failure associated with severe LV systolic dysfunction (HFpEF) versus normal LVEF. See text for discussion. CO, carbon dioxide; EDV, end-diastolic volume; ESV, end-systolic volume; PCWP, pulmonary capillary wedge pressure; RER, respiratory exchange ratio; SV, stroke volume. (Data from Refs.,,)
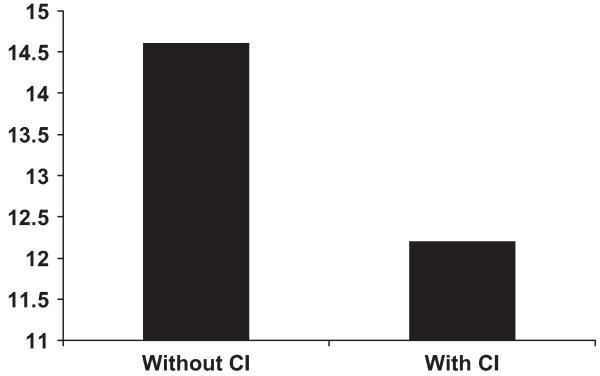
Peak exercise VO2 (y-axis, in mL/kg/min) in patients who have heart failure with and without chronotropic incompetence (CI). Patients who have chronotropic incompetence have more severe exercise intolerance, suggesting a contributory role for CI. (Adapted from Brubaker PH, Joo KC, Steward KP, et al. Chronotropic incompetence and its contribution to exercise intolerance in older heart failure patients. J Cardiopulm Rehab 2006;26:86-9; with permission.)
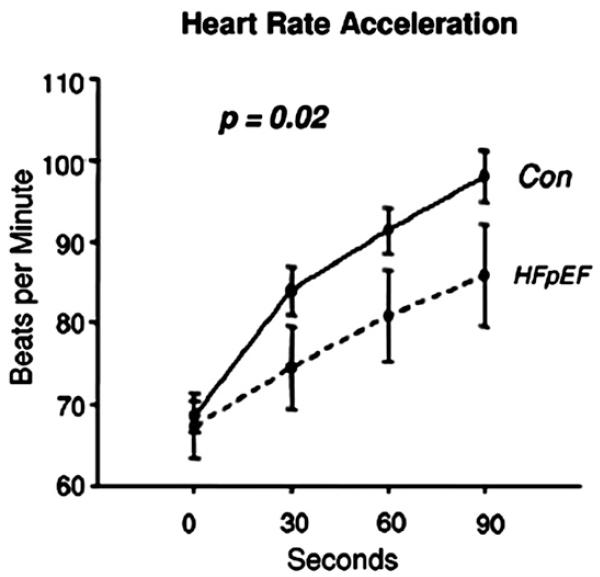
Heart rate acceleration during exercise in controls (Con) and patients who have heart failure and preserved EF (HFpEF). (From Borlaug BA, Melenovsky V, Russell SD, et al. Impaired chronotropic and vasodilator reserves limit exercise capacity in patients with heart failure and a preserved ejection fraction. Circulation 2006;114:2144; with permission.)
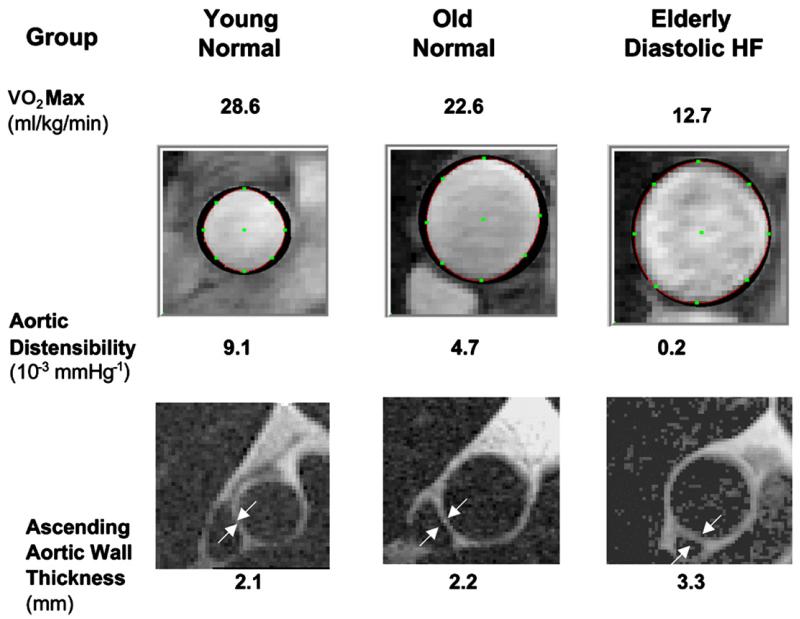
Data and images from representative subjects from healthy young persons, healthy elderly persons, and elderly patients who have diastolic heart failure (HF). Maximal exercise oxygen consumption (VO2max), aortic distensibility at rest, and the LV mass:volume ratio are shown. Patients who have DHF have severely reduced exercise tolerance (VO2max) and aortic distensibility and increased aortic wall thickness (arrows). (Adapted from Hundley WG, Kitzman DW, Morgan TM, et al. Cardiac cycle dependent changes in aortic area and aortic distensibility are reduced in older patients with isolated diastolic heart failure and correlate with exercise intolerance. J Am Coll Cardiol 2001;38(3):796-802; with permission. Copyright © 2001, American College of Cardiology.)
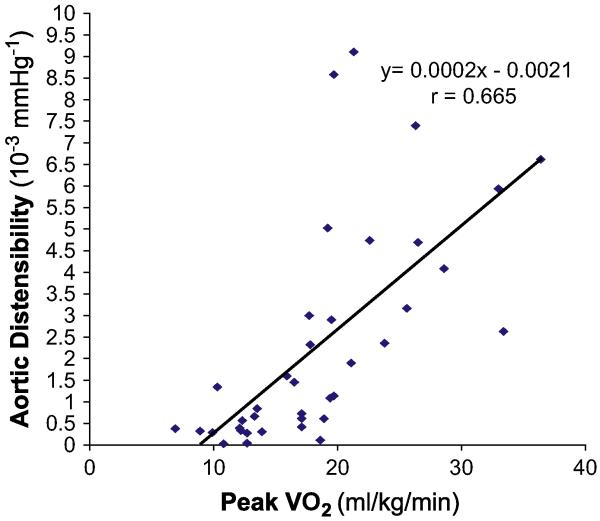
There is a close relationship between peak exercise VO2 (horizontal axis) and proximal aortic distensibility (vertical axis) in a group of 30 subjects (10 healthy young persons, 10 healthy elderly persons, and 10 elderly patients who have DHF). Each symbol represents the data from one participant. (From Hundley WG, Kitzman DW, Morgan TM, et al. Cardiac cycle dependent changes in aortic area and aortic distensibility are reduced in older patients with isolated diastolic heart failure and correlate with exercise intolerance. J Am Coll Cardiol 2001;38(3):796-802; with permission. Copyright © 2001, American College of Cardiology.)
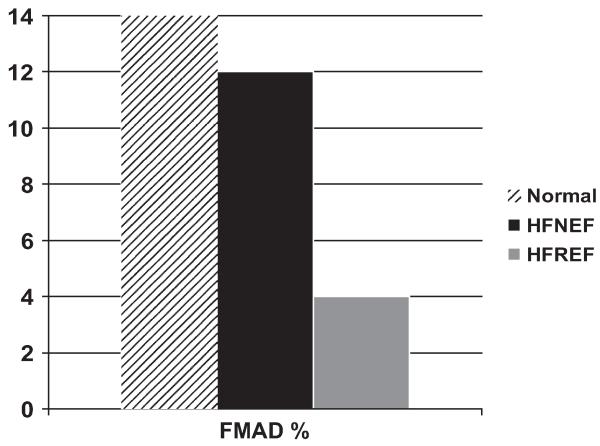
Flow-mediated arterial dilation (FMAD) of the femoral artery by phase-contrast MRI in normal subjects, elderly patients who have heart failure and normal EF (HFNEF), and patients who have heart failure and reduced EF (HFREF). FMAD is severely reduced in HFREF but is relatively preserved in HFNEF compared with age-matched healthy normal subjects. (From Hundley WG, Bayram E, Hamilton CA, et al. Leg flow-mediated arterial dilation in elderly patients with heart failure and normal left ventricular EF. Am J Physiol Heart Circ Physiol 2007;292(3):H1427-34; with permission.)
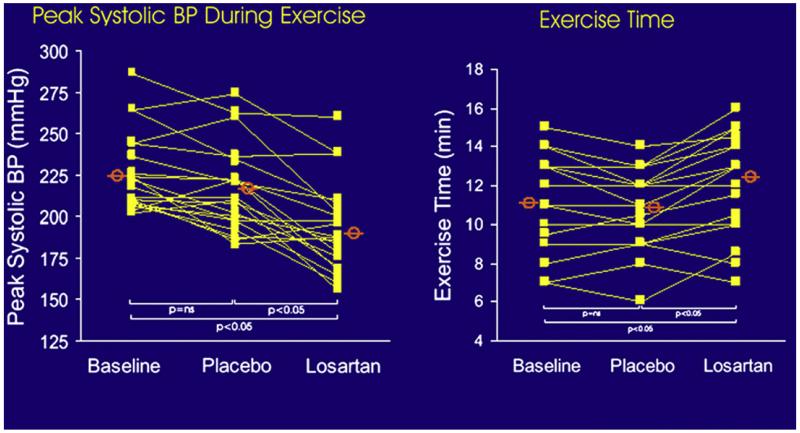
Plots of peak systolic blood pressure (BP) and exercise duration during baseline, during placebo administration, and during losartan administration in a randomized, controlled, cross-over trial. Treatment with the angiotensin II antagonist losartan increased exercise time. (From Warner JG, Metzger C, Kitzman DW, et al. Losartan improves exercise tolerance in patients with diastolic dysfunction and a hypertensive response to exercise. J Am Coll Cardiol 1999;33:1567-72; with permission. Copyright © 1999, American College of Cardiology.)
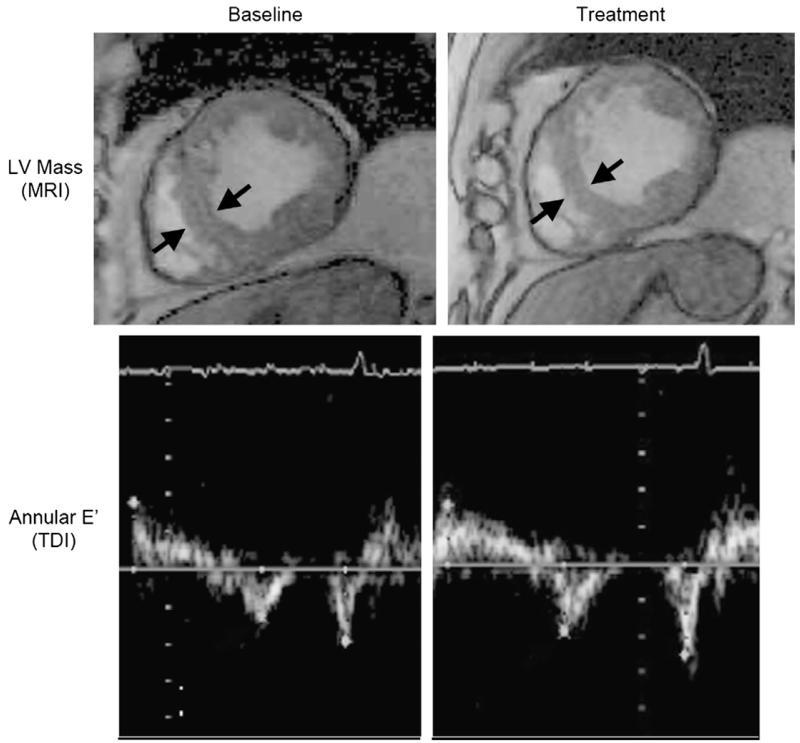
Effect of alagebrium on LV mass seen by MRI (top panel) and E′ seen by tissue Doppler imaging (TDI) in older patients who have DHF. (From Little WC, Zile MR, Kitzman DW, et al. The effect of alagebrium chloride (ALT-711), a novel glucose cross-link breaker, in the treatment of elderly patients with diastolic heart failure. J Card Fail 2005;11(3):191-5; with permission.)
Republished from
-
Exercise intolerance.Heart Fail Clin. 2008 Jan;4(1):99-115. doi: 10.1016/j.hfc.2007.12.002. Heart Fail Clin. 2008. PMID: 18313628 Free PMC article. Review.
References
-
- Gandhi SK, Powers JE, Fowle KM, et al. The pathogenesis of acute pulmonary edema associated with hypertension. N Engl J Med. 2000;344(1):17–22. - PubMed
-
- Powers JE, Gandhi SK, Kramer RK, et al. Predictors of poor outcome in patients with hypertensivepulmonary edema [abstract] J Am Coll Cardiol. 2004;43(5A):227A.
-
- Kitzman DW, Little WC, Brubaker PH, et al. Pathophysiological characterization of isolated diastolic heart failure in comparison to systolic heart failure. JAMA. 2002;288(17):2144–50. - PubMed
-
- Bol E, de Vries WR, Mosterd WL, et al. Cardiopulmonary exercise parameters in relation to all-cause mortality in patients with chronic heart failure. Int J Cardiol. 2000;72:255–63. - PubMed
-
- Jones RC, Francis GS, Lauer MS. Predictors of mortality in patients with heart failure and preserved systolic function in the Digitalis Investigation Group trial. J Am Coll Cardiol. 2004;44(5):1025–9. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
