

Design and powering of cystic fibrosis clinical trials using pulmonary exacerbation as an efficacy endpoint
- PMID: 21803665
- PMCID: PMC4079110
- DOI: 10.1016/j.jcf.2011.07.003
Design and powering of cystic fibrosis clinical trials using pulmonary exacerbation as an efficacy endpoint
Abstract
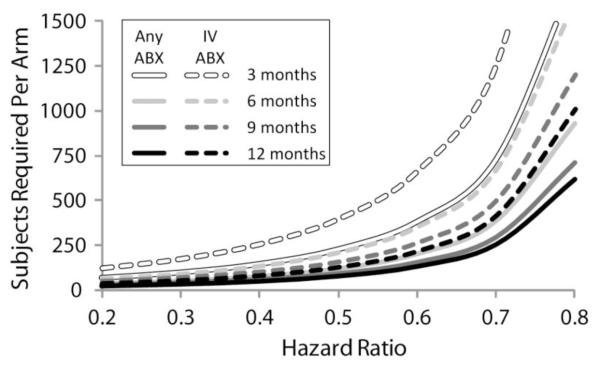
Background: Reduction in pulmonary exacerbations is an important efficacy endpoint for CF clinical studies. Powering exacerbation endpoints requires estimation of the future exacerbation incidence in CF study populations, but rates differ across the population.
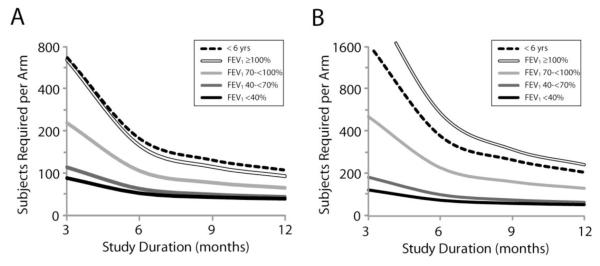
Methods: We have estimated exacerbation rates for Epidemiologic Study of CF subpopulations stratified by age, FEV(1)% predicted, sex, weight-for-age percentile, respiratory signs and symptoms, and history of exacerbation and bacterial culture. Sample sizes required to attain 80% power to detect exacerbation reductions of 20% to 80% in 1:1 randomized studies of 3 to 12 month duration were determined. Exacerbation treatments with "any" antibiotic (new oral quinolone, new inhaled antibiotic, or intravenous (IV) antibiotic) and with IV antibiotics were studied.
Results: At all ages, decreased FEV(1), female sex, exacerbation history, and Pseudomonas aeruginosa culture history were associated with increased treatment for exacerbation.
Conclusions: These data should assist investigators in the design of future CF exacerbation studies.
Copyright © 2011 European Cystic Fibrosis Society. Published by Elsevier B.V. All rights reserved.
Figures
References
-
- Ratjen F, Döring G. Cystic fibrosis. Lancet. 2003;361:681–9. REVIEW. - PubMed
-
- Ramsey BW. Management of pulmonary disease in patients with cystic fibrosis. N Engl J Med. 1996;335:179–88. Review. - PubMed
-
- Clinical Practice Guidelines for Cystic Fibrosis. Cystic Fibrosis Foundation; Bethesda, MD: 1997.
-
- Ferkol T, Rosenfeld M, Milla CE. Cystic fibrosis pulmonary exacerbations. J Pediatr. 2006;148:259–64. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
