

Endoscopic transthoracic limited sympathotomy for palmar-plantar hyperhidrosis: outcomes and complications during a 10-year period
- PMID: 21803954
- PMCID: PMC3146372
- DOI: 10.4065/mcp.2011.0199
Endoscopic transthoracic limited sympathotomy for palmar-plantar hyperhidrosis: outcomes and complications during a 10-year period
Erratum in
- Mayo Clin Proc. 2011 Nov;86(11):1126
Abstract
Objective: To review surgical results of endoscopic transthoracic limited sympathotomy for palmar-plantar hyperhidrosis during the past decade.
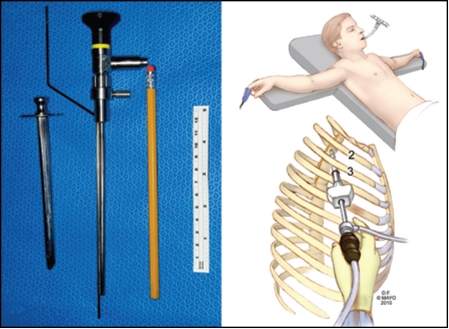
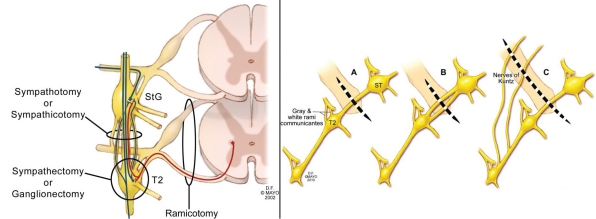
Patients and methods: We retrospectively reviewed 155 consecutive patients who underwent surgery from June 30, 2000, through December 31, 2009, for medically refractory palmar-plantar hyperhidrosis using a technique of T1-T2 sympathotomy disconnection, designed for successful palmar response and minimization of complications.
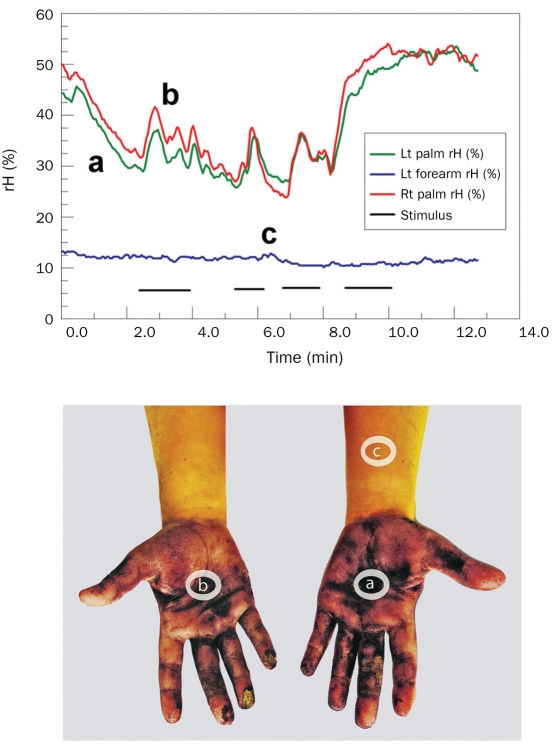
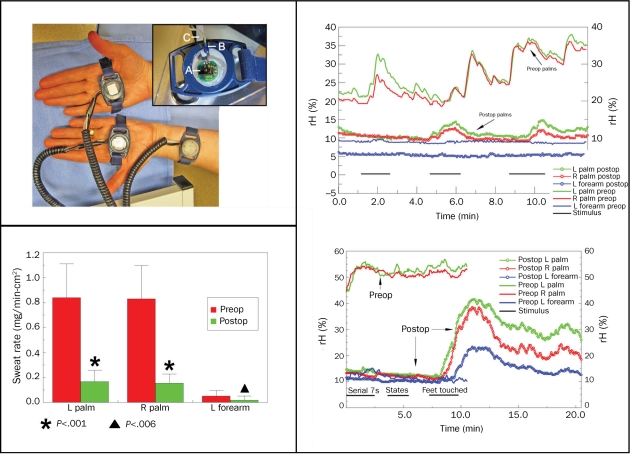
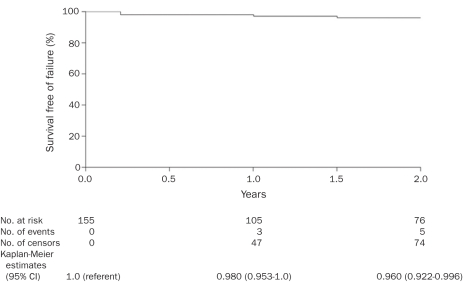
Results: Of the 155 patients, 44 (28.4%) were male, and 111 (71.6%) were female; operative times averaged 38 minutes. No patient experienced Horner syndrome, intercostal neuralgia, or pneumothorax. The only surgical complication was hemothorax in 2 patients (1.3%); in 1 patient, it occurred immediately postoperatively and in the other patient, 10 days postoperatively; treatment in both patients was successful. All 155 patients had successful (warm and dry) palmar responses at discharge. Long-term follow-up (>3 months; mean, 40.2 months) was obtained for 148 patients (95.5%) with the following responses to surgery: 96.6% of patients experienced successful control of palmar sweating; 69.2% of patients experienced decreased axillary sweating; and 39.8% of patients experienced decreased plantar sweating. At follow-up, 5 patients had palmar sweating (3 patients, <3 months; 1 patient, 10-12 months; 1 patient, 16-18 months). Compensatory hyperhidrosis did not occur in 47 patients (31.7%); it was mild in 92 patients (62.2%), moderate in 7 patients (4.7%), and severe in 2 patients (1.3%).
Conclusion: In this series, a small-diameter uniportal approach has eliminated intercostal neuralgia. Selecting a T1-T2 sympathotomy yields an excellent palmar response, with a very low severe compensatory hyperhidrosis complication rate. The low failure rate was noted during 18 months of follow-up and suggests that longer follow-up is necessary in these patients.
Figures
Comment in
-
The role of surgical treatment of hyperhidrosis.Mayo Clin Proc. 2011 Aug;86(8):717-8. doi: 10.4065/mcp.2011.0401. Mayo Clin Proc. 2011. PMID: 21803952 Free PMC article. No abstract available.
References
-
- Adson AW, Craig WM, Brown GE. Essential hyperhidrosis cured by sympathetic ganglionectomy and trunk resection. Arch Surg. 1935;31(5):794-806
-
- Kux E. The endoscopic approach to the vegetative nervous system and its therapeutic possibilities: especially in duodenal ulcer, angina pectoris, hypertension and diabetes. Dis Chest. 1951;20(2):139-147 - PubMed
-
- Vanaclocha V, Sáiz-Sapena N, Panta F. Uniportal endoscopic superior thoracic sympathectomy. Neurosurgery. 2000;46(4):924-928 - PubMed
-
- Steiner Z, Kleiner O, Hershkovitz Y, Mogilner J, Cohen Z. Compensatory sweating after thoracoscopic sympathectomy: an acceptable trade-off. J Pediatr Surg. 2007;42(7):1238-1242 - PubMed
-
- Chwajol M, Barrenechea IJ, Chakraborty S, Lesser JB, Connery CP, Perin NI. Impact of compensatory hyperhidrosis on patient satisfaction after endoscopic thoracic sympathectomy. Neurosurgery. 2009;64(3):511-518 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
