

Uremia alters HDL composition and function
- PMID: 21804091
- PMCID: PMC3171935
- DOI: 10.1681/ASN.2010111144
Uremia alters HDL composition and function
Abstract
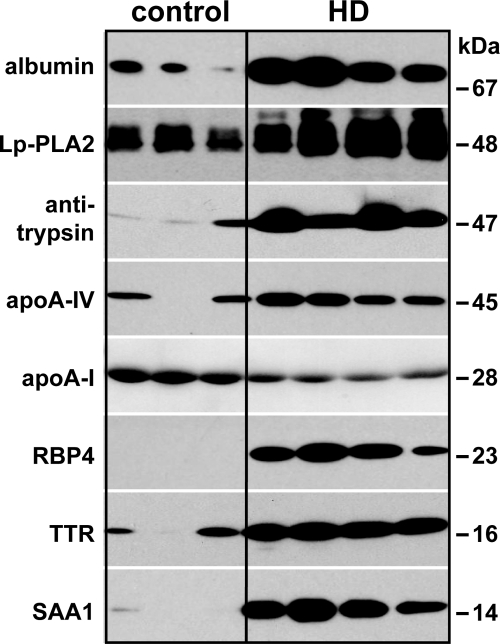
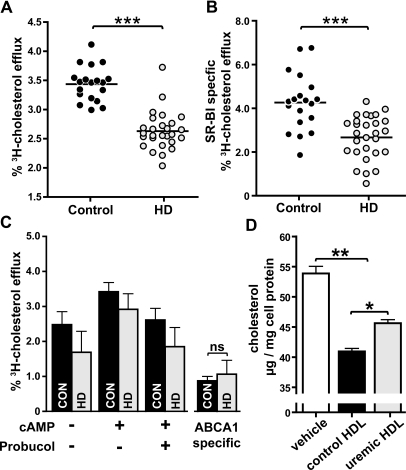
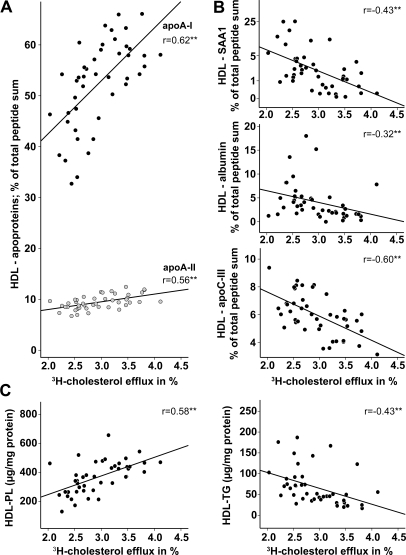
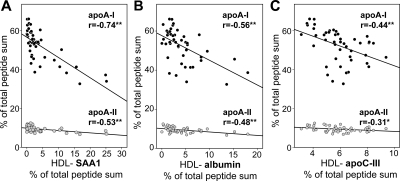
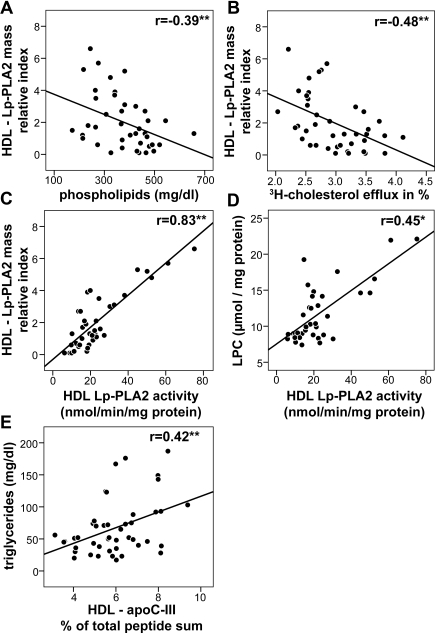
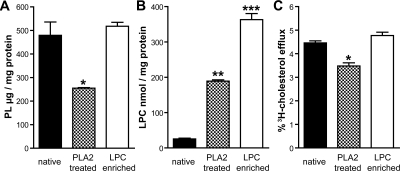
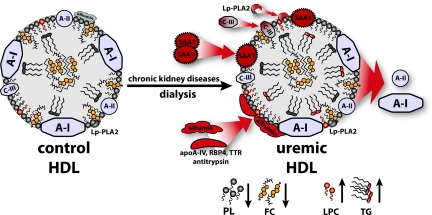
Functional impairment of HDL may contribute to the excess cardiovascular mortality experienced by patients with renal disease, but the effect of advanced renal disease on the composition and function of HDL is not well understood. Here, we used mass spectrometry and biochemical analyses to study alterations in the proteome and lipid composition of HDL isolated from patients on maintenance hemodialysis. We identified a significant increase in the amount of acute phase protein serum amyloid A1, albumin, lipoprotein-associated phospholipase A2, and apoC-III composing uremic HDL. Furthermore, uremic HDL contained reduced phospholipid and increased triglyceride and lysophospholipid. With regard to function, these changes impaired the ability of uremic HDL to promote cholesterol efflux from macrophages. In summary, the altered composition of HDL in renal disease seems to inhibit its cardioprotective properties. Assessing HDL composition and function in renal disease may help identify patients at increased risk for cardiovascular disease.
Figures
References
-
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY: Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med 351: 1296–1305, 2004 - PubMed
-
- Stenvinkel P: Chronic kidney disease: A public health priority and harbinger of premature cardiovascular disease. J Intern Med 268: 456–467, 2010 - PubMed
-
- Himmelfarb J, Stenvinkel P, Ikizler TA, Hakim RM: The elephant in uremia: Oxidant stress as a unifying concept of cardiovascular disease in uremia. Kidney Int 62: 1524–1538, 2002 - PubMed
-
- Stenvinkel P: Interactions between inflammation, oxidative stress, and endothelial dysfunction in end-stage renal disease. J Ren Nutr 13: 144–148, 2003 - PubMed
-
- Barter PJ, Nicholls S, Rye KA, Anantharamaiah GM, Navab M, Fogelman AM: Antiinflammatory properties of HDL. Circ Res 95: 764–772, 2004 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
