

Treatment strategies in severe symptomatic carotid and coronary artery disease
- PMID: 21804476
- PMCID: PMC3539602
- DOI: 10.12659/msm.881896
Treatment strategies in severe symptomatic carotid and coronary artery disease
Abstract
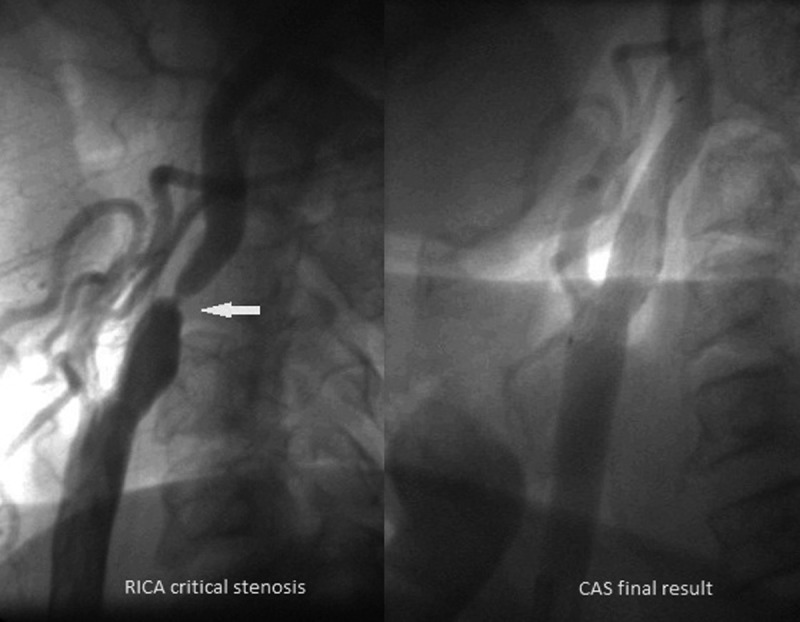
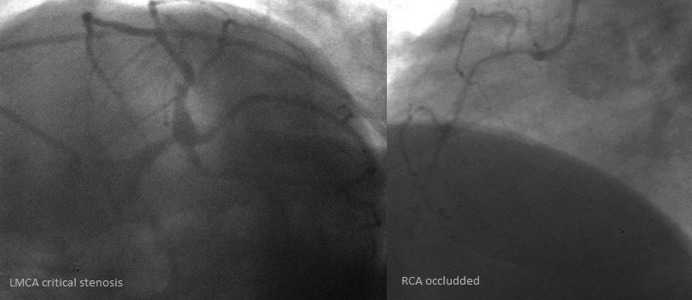
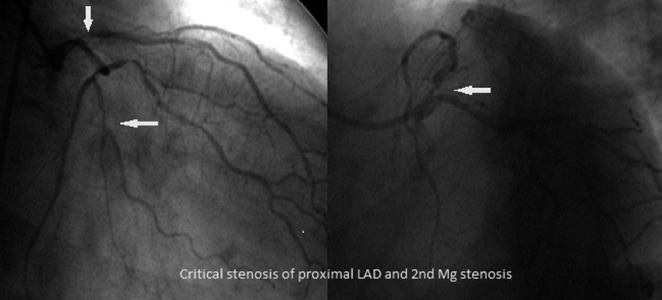
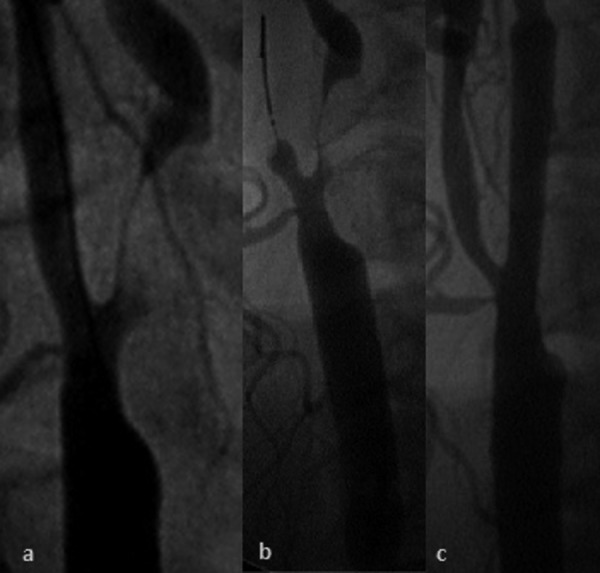
Coexistent carotid artery stenosis (CS) and multivessel coronary artery disease (CAD) is not infrequent. One in 5 patients with multivessel CAD has a severe CS, and CAD incidence reaches 80% in those referred for carotid revascularization. We reviewed treatment strategies for concomitant severe CS and CAD. We performed a literature search (MEDLINE) with terms including carotid artery stenting (CAS), coronary artery bypass grafting (CABG), carotid endarterectomy (CEA), stroke, and myocardial infarction (MI). The main therapeutic option for CS-CAD has been (simultaneous or staged) CEA-CABG. This, however, is associated with a high risk of MI (in those with CEA prior to CABG) or stroke (CABG prior to CEA), and the cumulative major adverse event rate (MAE - death, stroke or MI) reaches 10-12%. With increasing adoption of CAS, a sequential strategy of CAS followed by CABG has emerged. Registries (usually single-centre) indicate an MAE rate of ≈7% for CAS followed by CABG (frequently after >30 days, due to double antiplatelet therapy). Recently, 1-stage CAS-CABG has been introduced. This involves different antiplatelet regimens and, in some centers, preferred off-pump CABG, with a cumulative MAE of 1.4-4.5%. No randomized trial comparing different treatment strategies in CS-CAD has been conducted, and thus far reported series are prone to selection/reporting bias. In addition to the established surgical treatment (CEA-CABG, sequential/simultaneous), hybrid revascularization (CAS-CABG) is emerging as a viable therapeutic option. Larger, preferably multi-centre, studies are required before this can become widely applied.
Figures

References
-
- Hertzer NR, Loop FD, Beven EG, et al. Surgical staging for simultaneous coronary and carotid disease: a study including prospective randomization. J Vasc Surg. 1989;9(3):455–63. - PubMed
-
- Schwartz LB, Bridgman AH, Kieffer RW, et al. Asymptomatic carotid artery stenosis and stroke in patients undergoing cardiopulmonary bypass. J Vasc Surg. 1995;21(1):146–53. - PubMed
-
- Kallikazaros I, Tsioufis C, Sideris S, et al. Carotid artery disease as a marker for the presence of severe coronary artery disease in patients evaluated for chest pain. Stroke. 1999;30:1002–7. - PubMed
-
- Pieniazek P, Musialek P, Kablak-Ziembicka A, et al. Carotid artery stenting with patient- and lesion-tailored selection of the neuroprotection system and stent type: early and 5-year results from a prospective academic registry of 535 consecutive procedures (TARGET-CAS) J Endovasc Ther. 2008;15:249–262. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
