

A randomized trial of contingency management delivered in the context of group counseling
- PMID: 21806297
- PMCID: PMC3722591
- DOI: 10.1037/a0024813
A randomized trial of contingency management delivered in the context of group counseling
Abstract
Objective: Contingency management (CM) is efficacious in reducing drug use. Typically, reinforcers are provided on an individual basis to patients for submitting drug-negative samples. However, most treatment is provided in a group context, and poor attendance is a substantial concern. This study evaluated whether adding CM to group-based outpatient treatment would increase attendance and drug abstinence relative to standard care.
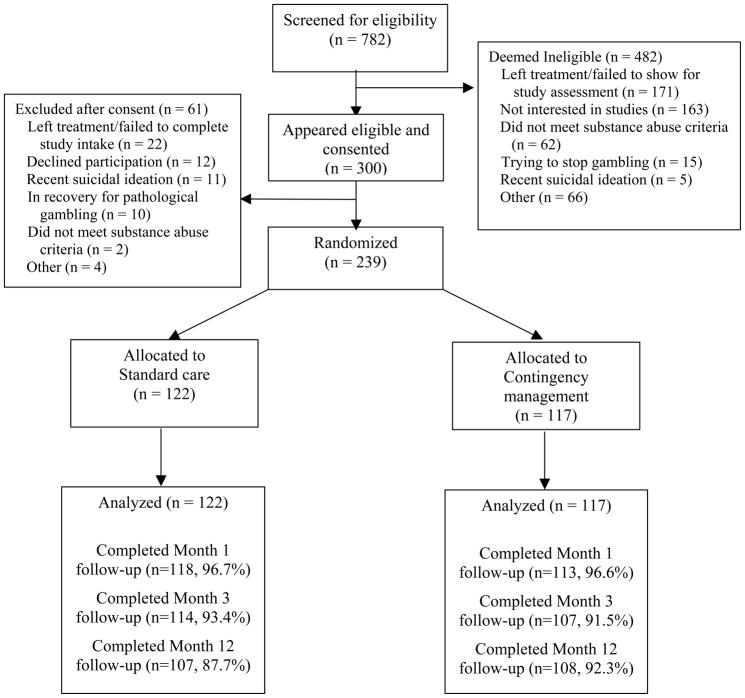
Method: Substance abusing patients (N = 239) initiating outpatient treatment at 2 community-based clinics were randomized to standard care with frequent urine sample monitoring for 12 weeks (SC) or that same treatment with CM delivered in the context of group counseling sessions. In the CM condition, patients earned opportunities to put their names in a hat based on attendance and submission of drug-negative samples. At group counseling sessions, therapists selected names randomly from the hat, and individuals whose names were drawn won prizes ranging from $1 to $100.
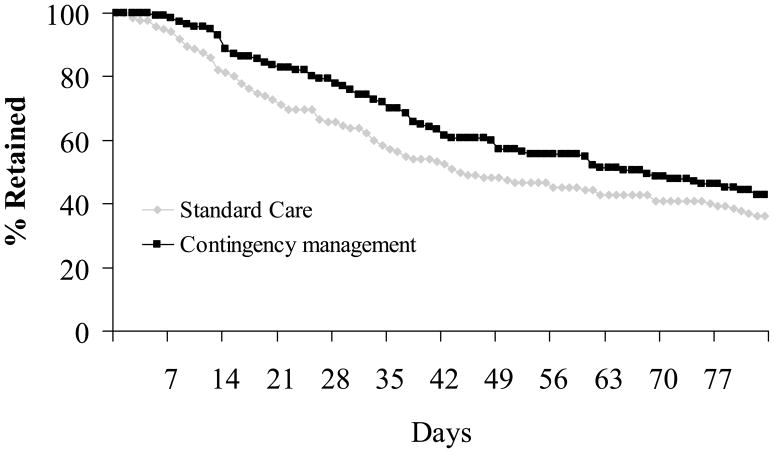
Results: Patients assigned to CM earned a median of $160 in prizes, and they attended significantly more days of treatment (d = 0.25), remained in treatment for more continuous weeks (d = 0.40), and achieved longer durations of drug abstinence (d = 0.26) than patients randomized to SC. Group adherence and therapeutic alliance also improved with CM. In addition, HIV risk behaviors were significantly lower in CM relative to SC patients during early phases of treatment and at the 12-month follow-up.
Conclusions: These data demonstrate that CM delivered in the context of outpatient group counseling can increase attendance and improve drug abstinence.
Figures
References
-
- Alessi SM, Hanson T, Tardif M, Petry NM. Low-cost contingency management in community substance abuse treatment settings: A transition to delivering incentives in group therapy. Experimental and Clinical Psychopharmacology. 2007;15:293–300. - PubMed
-
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4. Washington, DC: American Psychiatric Association; 2000. Text Revision.
-
- Barlow DH. Healthcare policy, psychotherapy research, and the future of psychotherapy. American Psychologist. 1996;51:1050–1058. - PubMed
-
- Bovasso GB, Alterman AI, Cacciloa JS, Cook TG. Predictive validity of the Addiction Severity Index's composite scores in the assessment of 2-year outcomes in a methadone maintenance population. Psychology of Addictive Behaviors. 2001;15:171–176. - PubMed
Publication types
MeSH terms
Grants and funding
- R01 DA013444/DA/NIDA NIH HHS/United States
- P30-DA023918/DA/NIDA NIH HHS/United States
- R01-DA018883/DA/NIDA NIH HHS/United States
- R01-DA024667/DA/NIDA NIH HHS/United States
- P50 DA009241/DA/NIDA NIH HHS/United States
- R01 DA024667/DA/NIDA NIH HHS/United States
- R01 DA018883/DA/NIDA NIH HHS/United States
- M01 RR006192/RR/NCRR NIH HHS/United States
- R01 DA016855/DA/NIDA NIH HHS/United States
- R01-DA022739/DA/NIDA NIH HHS/United States
- P60 AA003510/AA/NIAAA NIH HHS/United States
- R01-DA016855/DA/NIDA NIH HHS/United States
- R01-DA027615/DA/NIDA NIH HHS/United States
- R01-DA13444/DA/NIDA NIH HHS/United States
- R01 DA027615/DA/NIDA NIH HHS/United States
- R01 DA014618/DA/NIDA NIH HHS/United States
- R01 DA022739/DA/NIDA NIH HHS/United States
- M01-RR06192/RR/NCRR NIH HHS/United States
- R01-DA14618/DA/NIDA NIH HHS/United States
- P60-AA03510/AA/NIAAA NIH HHS/United States
- P30 DA023918/DA/NIDA NIH HHS/United States
- P50-DA09241/DA/NIDA NIH HHS/United States
