

COPD uncovered: an international survey on the impact of chronic obstructive pulmonary disease [COPD] on a working age population
- PMID: 21806798
- PMCID: PMC3163200
- DOI: 10.1186/1471-2458-11-612
COPD uncovered: an international survey on the impact of chronic obstructive pulmonary disease [COPD] on a working age population
Abstract
Background: Approximately 210 million people are estimated to have chronic obstructive pulmonary disease [COPD] worldwide. The burden of disease is known to be high, though less is known about those of a younger age. The aim of this study was to investigate the wider personal, economic and societal burden of COPD on a cross country working-age cohort.
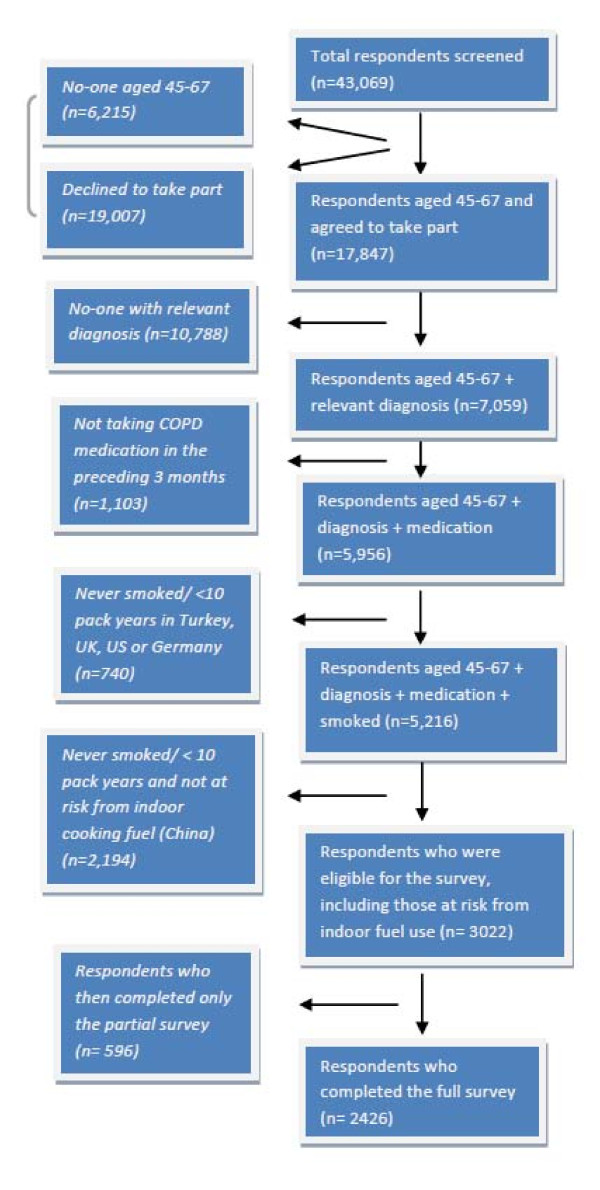
Methods: A cross-country [Brazil, China, Germany, Turkey, US, UK] cross-sectional survey methodology was utilised to answer the research questions. 2426 participants aged 45-67 recruited via a number of recruitment methods specific to each country completed the full survey. Inclusion criteria were a recalled physician diagnosis of COPD, a smoking history of > 10 pack years and the use of COPD medications in the previous 3 months prior to questioning. The survey included items from the validated Work Productivity and Activity Impairment [WPAI] scale and the EuroQoL 5 Dimension [EQ-5D] scale. Disease severity was measured using the 5-point MRC [Medical Research Council] dyspnoea scale as a surrogate measure.
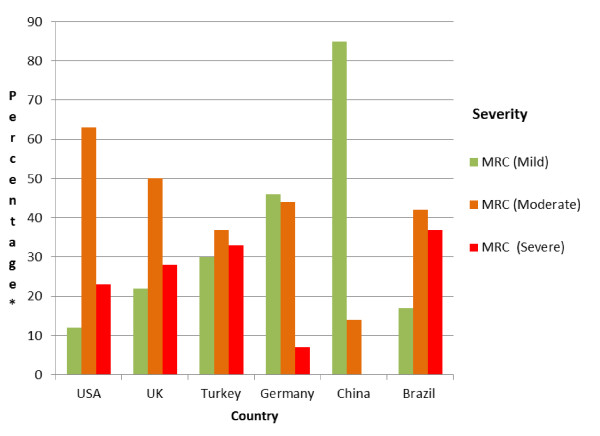
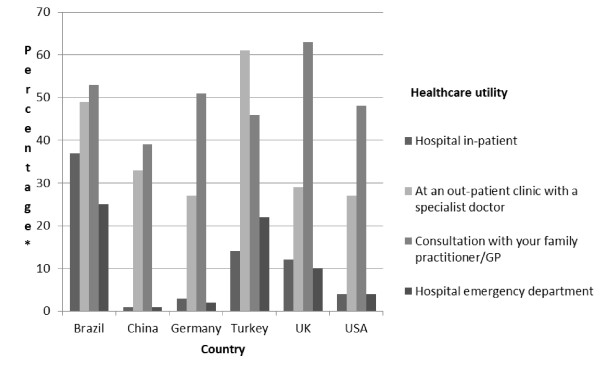
Results: 64% had either moderate [n = 1012] or severe [n = 521] COPD, although this varied by country. 75% of the cohort reported at least one comorbid condition. Quality of life declined with severity of illness [mild, mean EQ-5D score = 0.84; moderate 0.58; severe 0.41]. The annual cost of healthcare utilisation [excluding treatment costs and diagnostic tests] per individual was estimated to be $2,364 [£1,500]. For those remaining in active employment [n: 677]: lost time from work cost the individual an average of $880 [£556] per annum and lifetime losses of $7,365 [£4,661] amounting to $596,000 [£377,000] for the cohort. 447 [~40%] of the working population had retired prematurely because of COPD incurring individual estimated lifetime income losses of $316,000 [£200,000] or a combined total of $141 m [£89.6 m]. As the mean age of retirees was 58.3 and average time since retirement was 4 years, this suggests the average age of retirement is around 54. This would mean a high societal and economic impact in all study countries, particularly where typical state retirement ages are higher, for example in Brazil, Germany and the UK [65] and the US [65,66,67], compared to Turkey [58 for women, 60 for men] and China [60].
Conclusions: Although generalisation across a broader COPD population is limited due to the varied participant recruitment methods, these data nevertheless suggest that COPD has significant personal, economic and societal burden on working age people. Further efforts to improve COPD diagnosis and management are required.
Figures
References
-
- Lopez AD, Shibuya K, Rao C, Mathers CD, Hansell AL, Held LS. et al. Chronic obstructive pulmonary disease: current burden and future projections. EurRespirJ. 2006;27(2):397–412. - PubMed
-
- Halbert RJ, Natoli JL, Gano A, Badamgarav E, Buist AS, Mannino DM. Global burden of COPD: systematic review and meta-analysis. EurRespirJ. 2006;28(3):523–32. - PubMed
-
- Mannino DM, Braman S. The epidemiology and economics of chronic obstructive pulmonary disease. ProcAmThoracSoc. 2007;4(7):502–6. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
