

Decreased serum albumin as a biomarker for severe acute graft-versus-host disease after reduced-intensity allogeneic hematopoietic cell transplantation
- PMID: 21806949
- PMCID: PMC3203323
- DOI: 10.1016/j.bbmt.2011.07.021
Decreased serum albumin as a biomarker for severe acute graft-versus-host disease after reduced-intensity allogeneic hematopoietic cell transplantation
Abstract
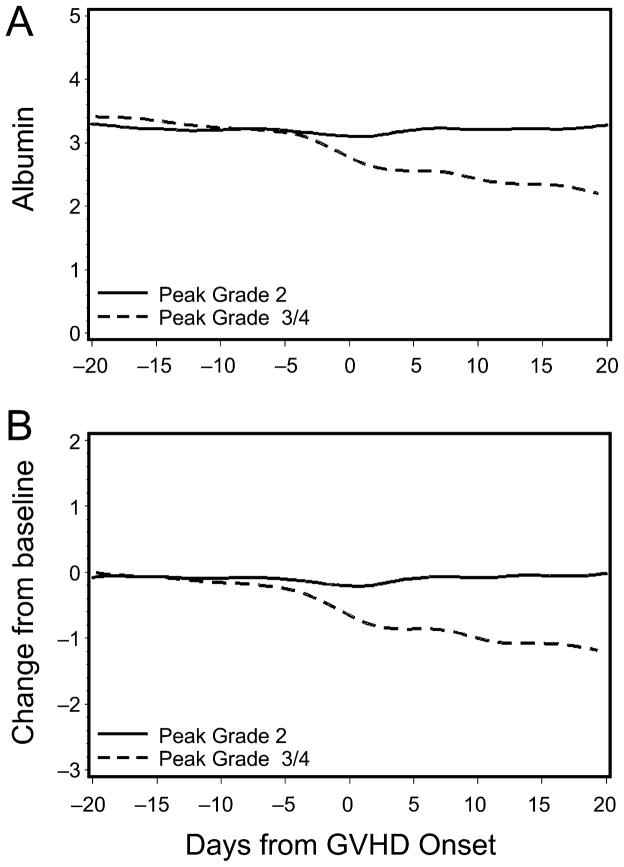
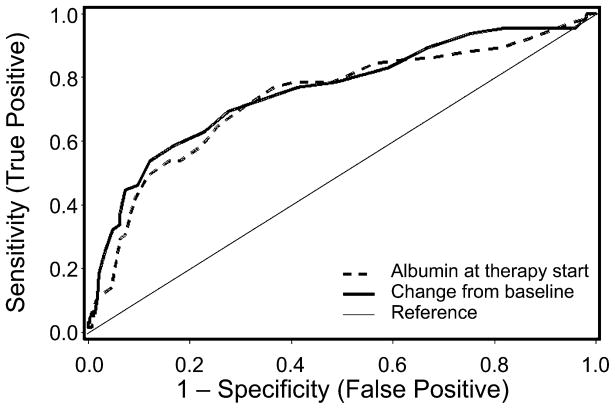
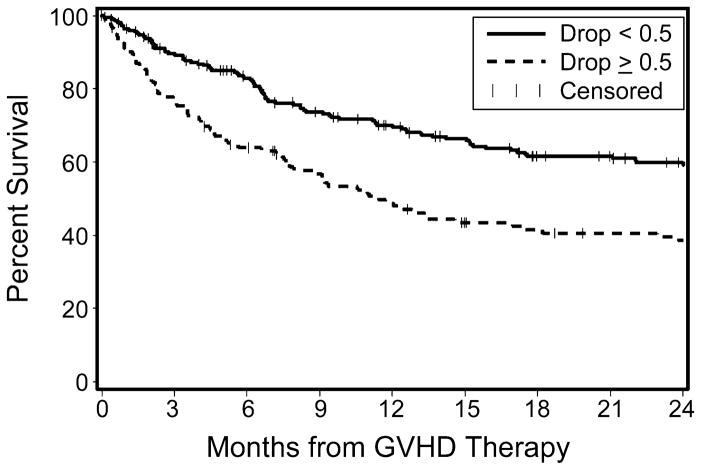
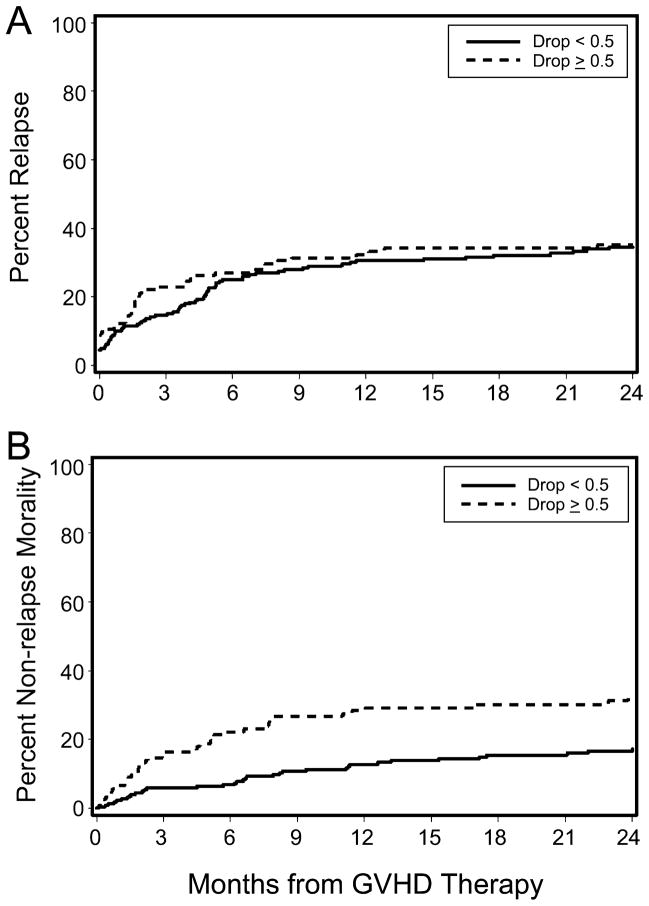
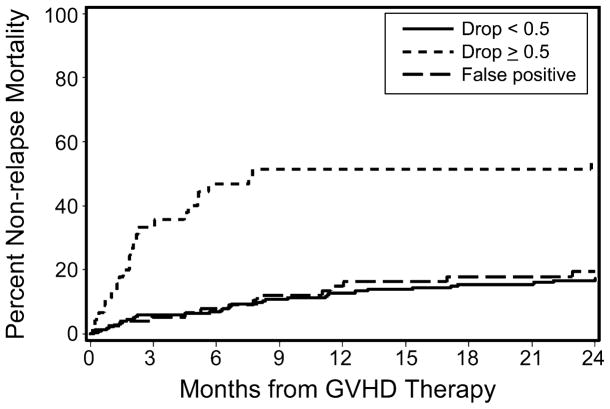
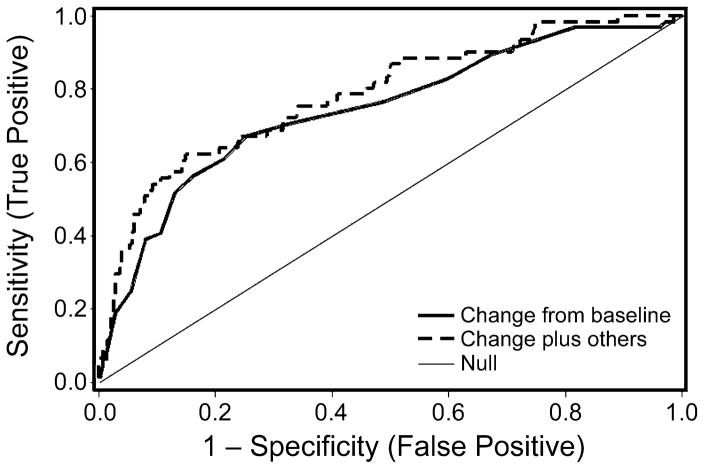
Biomarkers capable of predicting the onset and severity of acute graft-versus-host disease (aGVHD) after allogeneic hematopoietic cell transplantation (HCT) would enable preemptive and risk-stratified therapy. Severe aGVHD leads to gastrointestinal protein loss, resulting in hypoalbuminemia. We hypothesized that decreases in serum albumin at onset of aGVHD would predict the risk of progression to severe aGVHD. We identified 401 patients who developed aGVHD grades II-IV after reduced-intensity allogeneic HCT and reviewed all available serum albumin values from 30 days before HCT to 45 days after initiation of treatment for aGVHD. A ≥0.5 g/dL decrease in serum albumin concentration from pretransplantation baseline to the onset of treatment for aGVHD predicted the subsequent development of grade III/IV aGVHD (versus grade II aGVHD) with a sensitivity of 69% and a specificity of 73%. Overall mortality at 6 months after initiation of aGVHD treatment was 36% versus 17% for patients with and without ≥0.5 g/dL decreases in serum albumin, respectively (P = .0009). We conclude that change in serum albumin concentration from baseline to initiation of aGVHD treatment is an inexpensive, readily available, and predictive biomarker of GVHD severity and mortality after reduced-intensity allogeneic HCT.
Copyright © 2011 American Society for Blood and Marrow Transplantation. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Burroughs L, Mielcarek M, Leisenring W, et al. Extending postgrafting cyclosporine decreases the risk of severe graft-versus-host disease after nonmyeloablative hematopoietic cell transplantation. Transplantation. 2006;81:818–825. - PubMed
-
- Bacigalupo A, Lamparelli T, Milone G, et al. Pre-emptive treatment of acute GVHD: a randomized multicenter trial of rabbit anti-thymocyte globulin, given on day+7 after alternative donor transplants. Bone Marrow Transplant. 2010;45:385–391. - PubMed
-
- Sormani MP, Oneto R, Bruno B, et al. A revised day +7 predictive score for transplant-related mortality: serum cholinesterase, total protein, blood urea nitrogen, gamma glutamyl transferase, donor type and cell dose. Bone Marrow Transplant. 2003;32:205–211. - PubMed
-
- Lunn RA, Sumar N, Bansal AS, Treleaven J. Cytokine profiles in stem cell transplantation: possible use as a predictor of graft-versus-host disease. Hematology. 2005;10:107–114. - PubMed
-
- Mischak-Weissinger EM, Holler E, Schleuning M, et al. Prospective evaluation of an agvhd-specific proteomic patten in more than 340 patients. Blood. 2009;114:147. #347[abstr.]
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
