

Posttraumatic stress due to an acute coronary syndrome increases risk of 42-month major adverse cardiac events and all-cause mortality
- PMID: 21807378
- PMCID: PMC3210372
- DOI: 10.1016/j.jpsychires.2011.07.004
Posttraumatic stress due to an acute coronary syndrome increases risk of 42-month major adverse cardiac events and all-cause mortality
Abstract
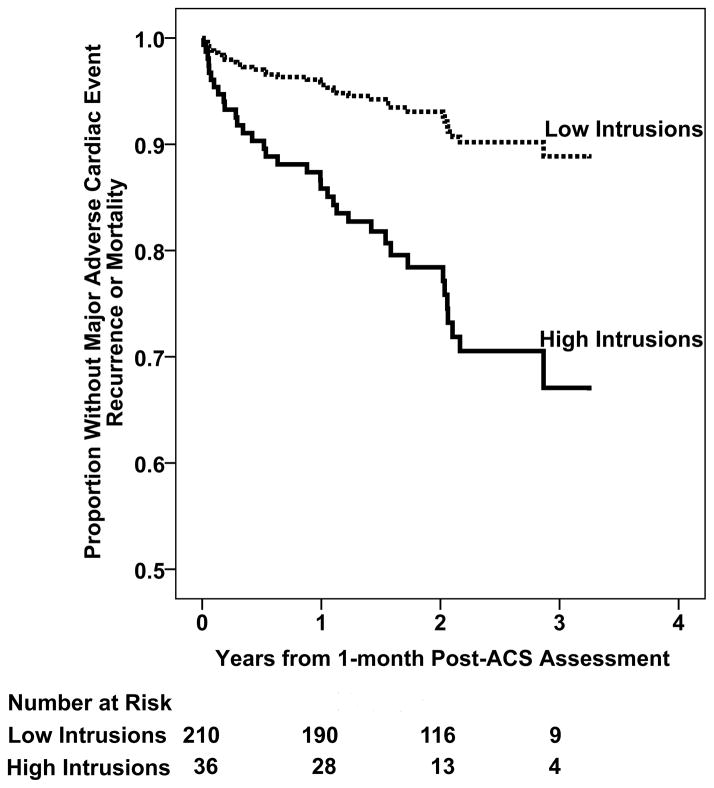
Approximately 15% of patients with acute coronary syndromes (ACS) develop posttraumatic stress disorder (PTSD) due to their ACS event. We assessed whether ACS-induced PTSD symptoms increase risk for major adverse cardiac events (MACE) and all-cause mortality (ACM) in an observational cohort study of 247 patients (aged 25-93 years; 45% women) hospitalized for an ACS at one of 3 academic medical centers in New York and Connecticut between November 2003 and June 2005. Within 1 week of admission, patient demographics, Global Registry of Acute Coronary Events risk score, Charlson comorbidity index, left ventricular ejection fraction, and depression status were obtained. At 1-month follow-up, ACS-induced PTSD symptoms were assessed with the Impact of Events Scale-Revised. The primary endpoint was combined MACE (hospitalization for myocardial infarction, unstable angina or urgent/emergency coronary revascularization procedures) and ACM, which were actively surveyed for 42 months after index event. Thirty-six (15%) patients had elevated intrusion symptoms, 32 (13%) elevated avoidance symptoms, and 21 (9%) elevated hyperarousal symptoms. Study physicians adjudicated 21 MACEs and 15 deaths during the follow-up period. In unadjusted Cox proportional hazards regression analyses, and analyses adjusted for sex, age, clinical characteristics and depression, high intrusion symptoms were associated with the primary endpoint (adjusted hazard ratio, 3.38; 95% confidence interval, 1.27-9.02; p = .015). Avoidance and hyperarousal symptoms were not associated with the primary endpoint. The presence of intrusion symptoms is a strong and independent predictor of elevated risk for MACE and ACM, and should be considered in the risk stratification of ACS patients.
Copyright © 2011 Elsevier Ltd. All rights reserved.
Figures
References
-
- Ayers S, Copland C, Dunmore E. A preliminary study of negative appraisals and dysfunctional coping associated with post-traumatic stress disorder symptoms following myocardial infarction. British Journal of Health Psychology. 2009;14:459–71. - PubMed
-
- Baum A, Cohen L, Hall M. Control and intrusive memories as possible determinants of chronic stress. Psychosomatic Medicine. 1993;55:274–86. - PubMed
-
- Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Archives of General Psychiatry. 1961;4:561–71. - PubMed
-
- Cannon CP, Battler A, Brindis RG, Cox JL, Ellis SG, Every NR, Flaherty JT, Harrington RA, Krumholz HM, Simoons ML, Van De Werf FJ, Weintraub WS, Mitchell KR, Morrisson SL, Anderson HV, Cannom DS, Chitwood WR, Cigarroa JE, Collins-Nakai RL, Gibbons RJ, Grover FL, Heidenreich PA, Khandheria BK, Knoebel SB, Krumholz HL, Malenka DJ, Mark DB, McKay CR, Passamani ER, Radford MJ, Riner RN, Schwartz JB, Shaw RE, Shemin RJ, Van Fossen DB, Verrier ED, Watkins MW, Phoubandith DR, Furnelli T. American College of Cardiology key data elements and definitions for measuring the clinical management and outcomes of patients with acute coronary syndromes. A report of the American College of Cardiology Task Force on Clinical Data Standards (Acute Coronary Syndromes Writing Committee) Journal of the American College of Cardiology. 2001;38:2114–30. - PubMed
-
- Charlson M, Szatrowski TP, Peterson J, Gold J. Validation of a combined comorbidity index. Journal of Clinical Epidemiology. 1994;47:1245–51. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
