

Acute localized administration of tetrahydrobiopterin and chronic systemic atorvastatin treatment restore cutaneous microvascular function in hypercholesterolaemic humans
- PMID: 21807618
- PMCID: PMC3213424
- DOI: 10.1113/jphysiol.2011.212100
Acute localized administration of tetrahydrobiopterin and chronic systemic atorvastatin treatment restore cutaneous microvascular function in hypercholesterolaemic humans
Abstract
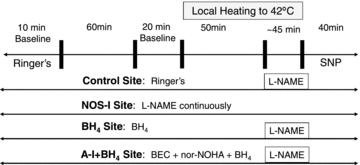
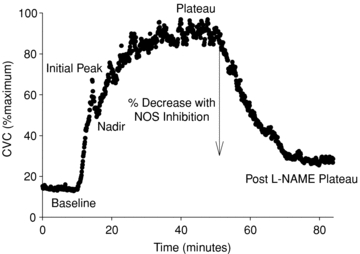
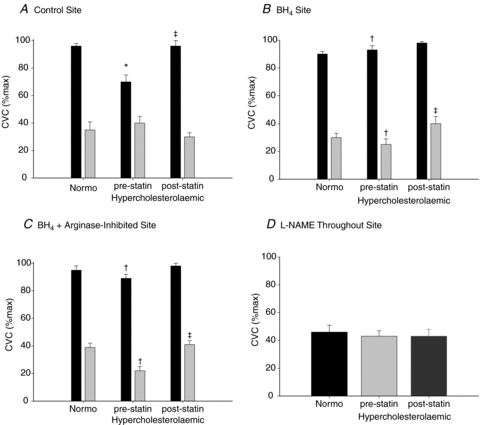
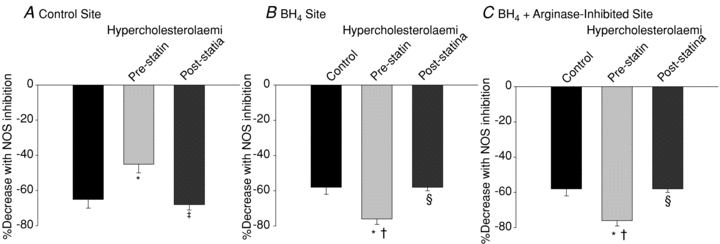
Elevated oxidized low-density lipoproteins (LDL) are associated with vascular dysfunction in the cutaneous microvasculature, induced in part by upregulated arginase activity and increased globalized oxidant stress. Since tetrahydrobiopterin (BH(4)) is an essential cofactor for endothelial nitric oxide synthase (NOS3), decreased bioavailability of the substrate l-arginine and/or BH(4) may contribute to decreased NO production with hypercholesterolaemia. We hypothesized that (1) localized administration of BH(4) would augment NO-dependent vasodilatation in hypercholesterolaemic human skin, which would be further increased when combined with arginase inhibition and (2) the improvement induced by localized BH(4) would be attenuated after a 3 month oral atorvastatin intervention (10 mg). Four microdialysis fibres were placed in the skin of nine normocholesterolaemic (NC: LDL = 95 ± 4 mg dl(-1)) and nine hypercholesterolaemic (HC: LDL = 177 ± 6 mg dl(-1)) men and women before and after 3 months of systemic atorvastatin. Sites served as control, NOS inhibited, BH(4), and arginase inhibited + BH(4) (combo). Skin blood flow was measured while local skin heating (42°C) induced NO-dependent vasodilatation. After the established plateau l-NAME was perfused in all sites to quantify NO-dependent vasodilatation (NO). Data were normalized to maximum cutaneous vascular conductance (CVC). Vasodilatation at the plateau and NO-dependent vasodilatation were reduced in HC subjects (plateau HC: 70 ± 5% CVC(max) vs. NC: 95 ± 2% CVC(max); NO HC: 45 ± 5% CVC(max) vs. NC: 64 ± 5% CVC(max); both P < 0.001). Localized BH(4) alone or combo augmented the plateau (BH(4): 93 ± 3% CVC(max); combo 89 ± 3% CVC(max), both P < 0.001) and NO-dependent vasodilatation in HC (BH(4): 74 ± 3% CVC(max); combo 76 ± 3% CVC(max), both P < 0.001), but there was no effect in NC subjects (plateau BH(4): 90 ± 2% CVC(max); combo 95 ± 3% CVC(max); NO-dependent vasodilatation BH(4): 68 ± 3% CVC(max); combo 58 ± 4% CVC(max), all P > 0.05 vs. control site). After the atorvastatin intervention (LDL = 98 ± mg * dl(-1)) there was an increase in the plateau in HC (96 ± 4% CVC(max), P < 0.001) and NO-dependent vasodilatation (68 ± 3% CVC(max), P < 0.001). Localized BH(4) alone or combo was less effective at increasing NO-dependent vasodilatation after the drug intervention (BH(4): 60 ± 5% CVC(max); combo 58 ± 2% CVC(max), both P < 0.001). These data suggest that decreased BH(4) bioavailability contributes in part to cutaneous microvascular dysfunction in hypercholesterolaemic humans and that atorvastatin is an effective systemic treatment for improving NOS coupling mechanisms in the microvasculature.
Figures
References
-
- Ash DE. Structure and function of arginases. J Nutr. 2004;134:2760S–2764S. discussion 2765S-2767S. - PubMed
-
- Bailey SR, Eid AH, Mitra S, Flavahan S, Flavahan NA. Rho kinase mediates cold-induced constriction of cutaneous arteries: role of α2C-adrenoceptor translocation. Circ Res. 2004;94:1367–1374. - PubMed
-
- Bendall JK, Alp NJ, Warrick N, Cai S, Adlam D, Rockett K, et al. Stoichiometric relationships between endothelial tetrahydrobiopterin, endothelial NO synthase (eNOS) activity, and eNOS coupling in vivo: insights from transgenic mice with endothelial-targeted GTP cyclohydrolase 1 and eNOS overexpression. Circ Res. 2005;97:864–871. - PubMed
-
- Berkowitz DE, White R, Li D, Minhas KM, Cernetich A, Kim S, et al. Arginase reciprocally regulates nitric oxide synthase activity and contributes to endothelial dysfunction in aging blood vessels. Circulation. 2003;108:2000–2006. - PubMed
-
- Cosentino F, Hurlimann D, Delli Gatti C, Chenevard R, Blau N, Alp NJ, Channon KM, Eto M, Lerch P, Enseleit F, Ruschitzka F, Volpe M, Luscher TF, Noll G. Chronic Treatment with Tetrahydrobiopterin Reverses Endothelial Dysfunction and Oxidative Stress in Hypercholesterolemia. Heart. 2008;94:487–492. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical