

Chronic dysimmune neuropathies: Beyond chronic demyelinating polyradiculoneuropathy
- PMID: 21808468
- PMCID: PMC3141494
- DOI: 10.4103/0972-2327.82789
Chronic dysimmune neuropathies: Beyond chronic demyelinating polyradiculoneuropathy
Abstract
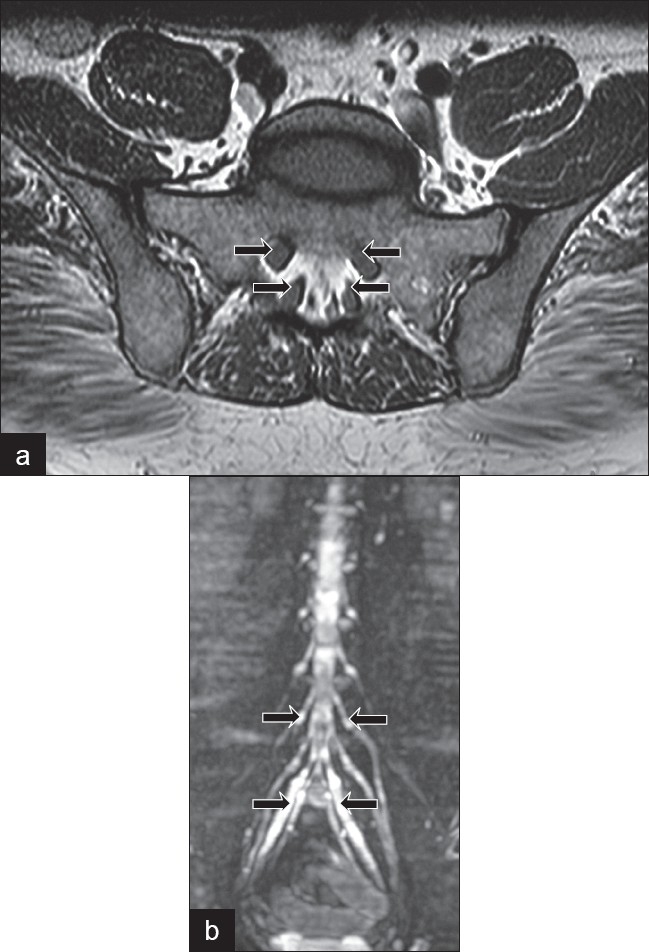
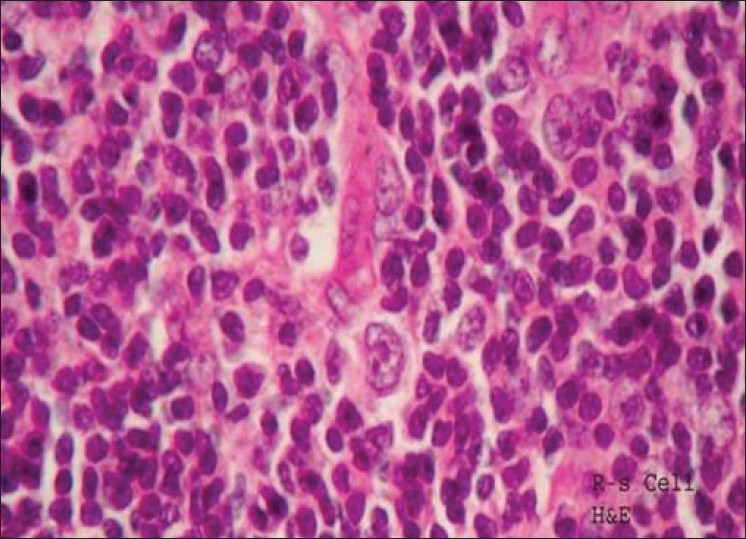
The spectrum of chronic dysimmune neuropathies has widened well beyond chronic demyelinating polyradiculoneuropathy (CIDP). Pure motor (multifocal motor neuropathy), sensorimotor with asymmetrical involvement (multifocal acquired demylinating sensory and motor neuropathy), exclusively distal sensory (distal acquired demyelinating sensory neuropathy) and very proximal sensory (chronic immune sensory polyradiculopathy) constitute the variants of CIDP. Correct diagnosis of these entities is of importance in terms of initiation of appropriate therapy as well as prognostication of these patients. The rates of detection of immune-mediated neuropathies with monoclonal cell proliferation (monoclonal gammopathy of unknown significance, multiple myeloma, etc.) have been facilitated as better diagnostic tools such as serum immunofixation electrophoresis are being used more often. Immune neuropathies associated with malignancies and systemic vasculitic disorders are being defined further and treated early with better understanding of the disease processes. As this field of dysimmune neuropathies will evolve in the future, some of the curious aspects of the clinical presentations and response patterns to different immunosuppressants or immunomodulators will be further elucidated. This review also discusses representative case studies.
Keywords: Multifocal motor neuropathy; chronic inflammatory demyelinating neuropathy; distal acquired demyelinating predominately sensory; multifocal acquired demyelinating sensory and motor.
Conflict of interest statement
Figures
References
-
- Roth G, Rohr J, Magistris MR, Ochsner F. Motor neuropathy with proximal multifocal persistent conduction block, fasciculations and myokymia. Evolution to tetraplegia. Eur Neurol. 1986;25:416–23. - PubMed
-
- Chad DA, Hammer K, Sargent J. Slow resolution of multifocal weakness and fasciculation: A reversible motor neuron syndrome. Neurology. 1986;36:1260–3. - PubMed
-
- Pestronk A, Cornblath DR, Ilyas AA, Baba H, Quarles RH, Griffin JW, et al. A treatable multifocal motor neuropathy with antibodies to GM1 ganglioside. Ann Neurol. 1988;24:73–8. - PubMed
-
- Van Asseldonk JT, Franssen H, Van den Berg-Vos RM, Wokke JH, Van den Berg LH. Multifocal motor neuropathy. Lancet Neurol. 2005;4:309–19. - PubMed
-
- Nobile-Orazio E. What's new in multifocal motor neuropathy in 2007–2008? J Peripher Nerv Syst. 2008;13:261–3. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
