

Dynamic plate osteosynthesis for fracture stabilization: how to do it
- PMID: 21808699
- PMCID: PMC3143947
- DOI: 10.4081/or.2010.e4
Dynamic plate osteosynthesis for fracture stabilization: how to do it
Abstract
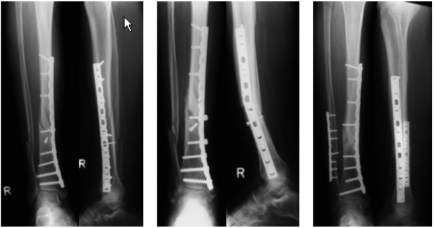
Plate osteosynthesis is one treatment option for the stabilization of long bones. It is widely accepted to achieve bone healing with a dynamic and biological fixation where the perfusion of the bone is left intact and micromotion at the fracture gap is allowed. The indications for a dynamic plate osteosynthesis include distal tibial and femoral fractures, some midshaft fractures, and adolescent tibial and femoral fractures with not fully closed growth plates. Although many lower limb shaft fractures are managed successfully with intramedullary nails, there are some important advantages of open-reduction-and-plate fixation: the risk of malalignment, anterior knee pain, or nonunion seems to be lower. The surgeon performing a plate osteosynthesis has the possibility to influence fixation strength and micromotion at the fracture gap. Long plates and oblique screws at the plate ends increase fixation strength. However, the number of screws does influence stiffness and stability. Lag screws and screws close to the fracture site reduce micromotion dramatically.DYNAMIC PLATE OSTEOSYNTHESIS CAN BE ACHIEVED BY APPLYING SOME SIMPLE RULES: long plates with only a few screws should be used. Oblique screws at the plate ends increase the pullout strength. Two or three holes at the fracture site should be omitted. Lag screws, especially through the plate, must be avoided whenever possible. Compression is not required. Locking plates are recommended only in fractures close to the joint. When respecting these basic concepts, dynamic plate osteosynthesis is a safe procedure with a high healing and a low complication rate.
Keywords: bone healing; dynamic osteosynthesis; fracture stabilization; plate fixation..
Conflict of interest statement
Conflict of interest: the authors report no conflicts of interest.
Figures






References
-
- Weber BG. Stuttgart: Thieme;; 2004. Minimax fracture fixation.
-
- Gerber C, Mast JW, Ganz R. Biological internal fixation of fractures. Arch Orthop Trauma Surg. 1990;109:295–303. - PubMed
-
- Aro HT, Chao EY. Bone-healing patterns affected by loading, fracture fragment stability, fracture type, and fracture site compression. Clin Orthop Relat Res. 1993;293:8–17. - PubMed
-
- Claes L, Heitemeyer U, Krischak G, et al. Fixation technique influences osteogenesis of comminuted fractures. Clin Orthop Relat Res. 1999;365:221–9. - PubMed
-
- Papakostidis C, Grotz MR, Papadokostakis G, et al. Femoral biologic plate fixation. Clin Orthop Relat Res. 2006;450:193–202. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous