

Arthroplasty of a Charcot knee
- PMID: 21808708
- PMCID: PMC3143972
- DOI: 10.4081/or.2010.e17
Arthroplasty of a Charcot knee
Abstract
The Charcot knee - or neuropathic arthropathy - presents a considerable challenge to the orthopaedic surgeon. Caused by a combination of sensory, motor and autonomic neuropathy, it was originally described as an arthritic sequelae of neurosyphilis. In today's western orthopaedics it is more often caused by diabetes. A Charcot knee is often symptomatically painful and unstable. Traditional management has usually been conservative or arthrodesis, with limited success. Arthroplasty of a Charcot joint has commonly been avoided at all costs. However, in the right patient, using the right technique, arthroplasty can significantly improve the symptoms of a Charcot joint. This article explores the evidence surrounding the role of arthroplasty in the management of a Charcot knee. Arthroplasty is compared to other forms of treatment and specific patient demographics and surgical techniques are explored in an attempt to define the role of arthroplasty in the management of a Charcot knee.
Keywords: Charcot joint; arthroplasty; knee; neuropathic arthropathy..
Conflict of interest statement
Conflicts of interest: the authors report no conflict of interest.
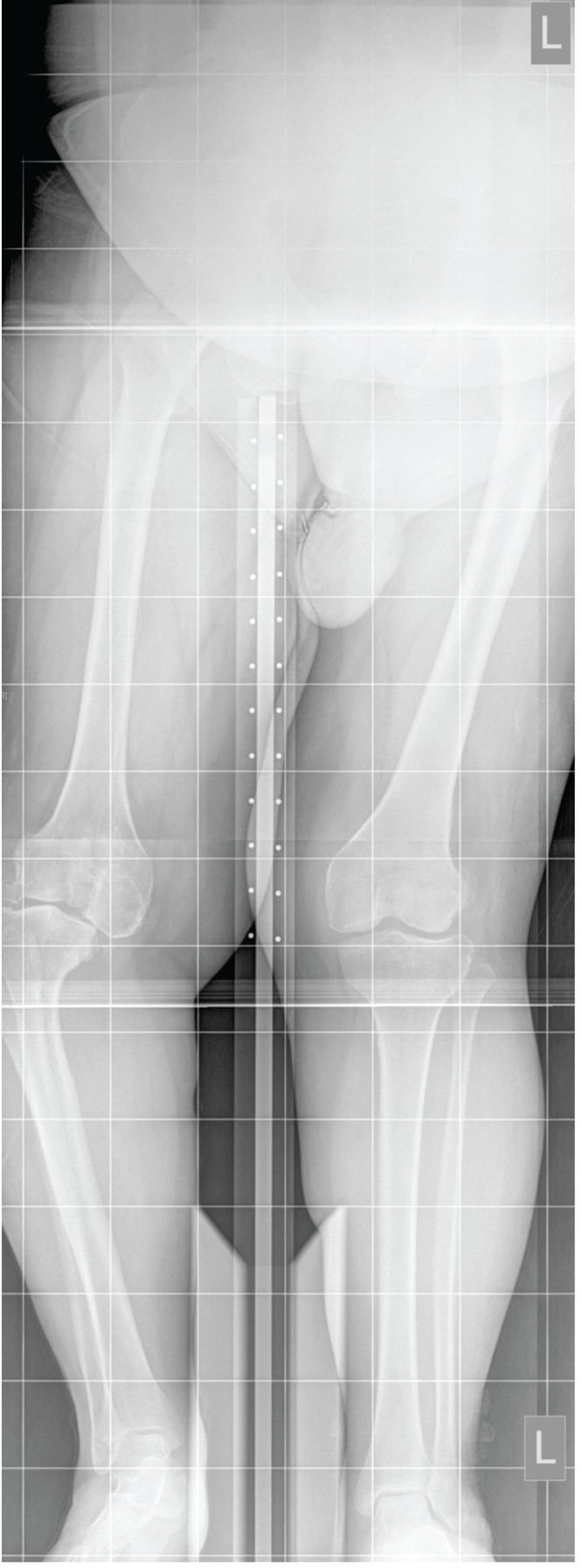
Figures




Similar articles
-
Charcot osteoarthropathy of the knee secondary to neurosyphilis: a rare condition managed by a challenging arthrodesis.BMJ Case Rep. 2018 Aug 20;2018:bcr2018225337. doi: 10.1136/bcr-2018-225337. BMJ Case Rep. 2018. PMID: 30131415 Free PMC article.
-
Arthroplasty of a Charcot Knee in a Patient With Congenital Insensitivity to Pain.Cureus. 2022 Apr 13;14(4):e24116. doi: 10.7759/cureus.24116. eCollection 2022 Apr. Cureus. 2022. PMID: 35573589 Free PMC article.
-
Neuropathic (Charcot) Arthropathy of the Knee.J Am Acad Orthop Surg. 2021 Dec 1;29(23):e1159-e1166. doi: 10.5435/JAAOS-D-21-00482. J Am Acad Orthop Surg. 2021. PMID: 34437307
-
Case report: Neuropathic arthropathy of the hip as a sequela of undiagnosed tertiary syphilis.Clin Orthop Relat Res. 2010 Nov;468(11):3126-31. doi: 10.1007/s11999-010-1257-0. Epub 2010 Feb 12. Clin Orthop Relat Res. 2010. PMID: 20151233 Free PMC article. Review.
-
Arthrodesis of the Charcot foot and ankle.Clin Podiatr Med Surg. 2004 Apr;21(2):271-89. doi: 10.1016/j.cpm.2004.01.007. Clin Podiatr Med Surg. 2004. PMID: 15063884 Review.
Cited by
-
Constrained Condylar Prostheses for the Treatment of Charcot Arthropathy: A Case Report and Literature Review.Orthop Surg. 2023 May;15(5):1423-1430. doi: 10.1111/os.13686. Epub 2023 Mar 1. Orthop Surg. 2023. PMID: 36859755 Free PMC article. Review.
-
Idiopathic Charcot Arthropathy of the Knee Presenting as a Bicondylar Tibial Plateau Fracture.J Am Acad Orthop Surg Glob Res Rev. 2018 Jul 17;2(7):e032. doi: 10.5435/JAAOSGlobal-D-18-00032. eCollection 2018 Jul. J Am Acad Orthop Surg Glob Res Rev. 2018. PMID: 30280143 Free PMC article.
-
Total knee arthroplasty in patients with Charcot joints.Knee Surg Sports Traumatol Arthrosc. 2016 Aug;24(8):2672-7. doi: 10.1007/s00167-016-4073-6. Epub 2016 Mar 26. Knee Surg Sports Traumatol Arthrosc. 2016. PMID: 27017217
-
Diabetic Neuropathic Arthropathy of the Knee: Two Case Reports and a Review of the Literature.Case Rep Orthop. 2018 Jan 23;2018:9301496. doi: 10.1155/2018/9301496. eCollection 2018. Case Rep Orthop. 2018. PMID: 29610694 Free PMC article.
-
Mid- to long-term outcomes of contemporary total knee arthroplasty in Charcot neuroarthropathy: a systematic review and meta-analysis.EFORT Open Rev. 2021 Jul 8;6(7):556-564. doi: 10.1302/2058-5241.6.200103. eCollection 2021 Jul. EFORT Open Rev. 2021. PMID: 34377547 Free PMC article. Review.
References
-
- Brower AC, Allman RM. Pathogenesis of the neurotrophic joint: neurotraumatic vs. neurovascular. Radiology. 1981;139:349–54. - PubMed
-
- Allman RM, Brower AC, Kotlyarov EB. Neuropathic bone and joint disease. Radiol Clin North Am. 1988;26:1373–81. - PubMed
-
- Hanft JR, Goggin JP, Landsman A, Surprenant M. The role of combined magnetic field bone growth stimulation as an adjunct in the treatment of neuroarthropathy/Charcot joint: an expanded pilot study. J Foot Ankle Surg. 1998;37:510–5. - PubMed
-
- Archer AG, Roberts VC, Watkins PJ. Blood flow patterns in painful diabetic neuropathy. Diabetologia. 1984;27:563–7. - PubMed
LinkOut - more resources
Full Text Sources