

Age-associated changes in cardiovascular structure and function: a fertile milieu for future disease
- PMID: 21809160
- PMCID: PMC4677819
- DOI: 10.1007/s10741-011-9270-2
Age-associated changes in cardiovascular structure and function: a fertile milieu for future disease
Abstract
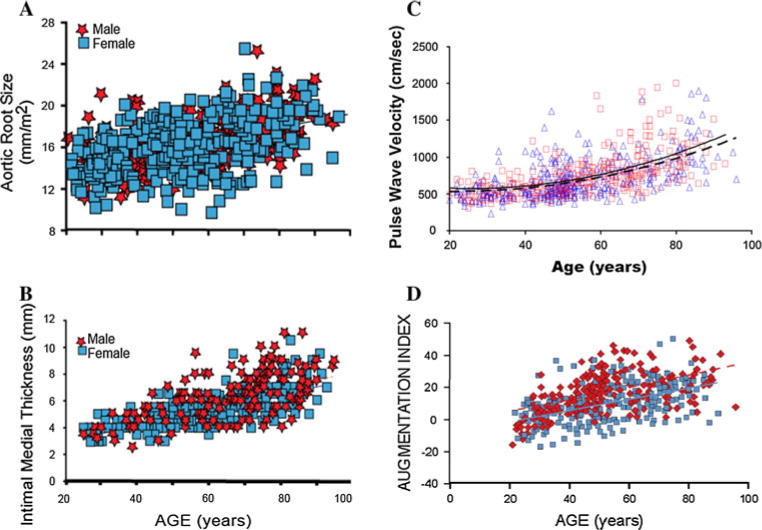
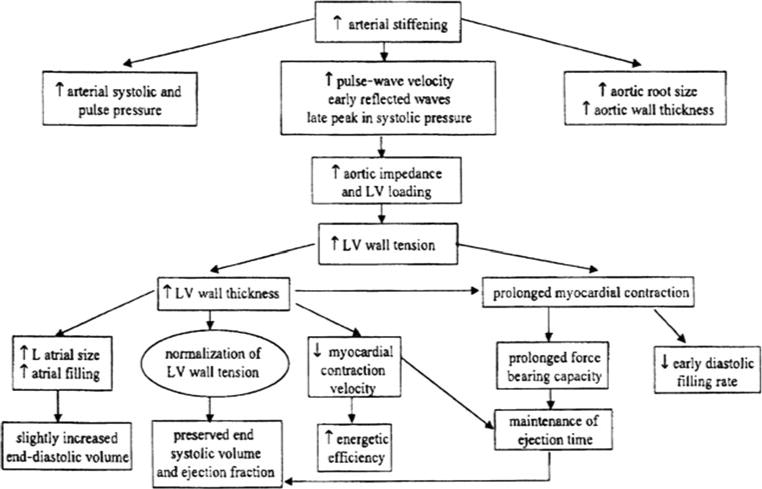
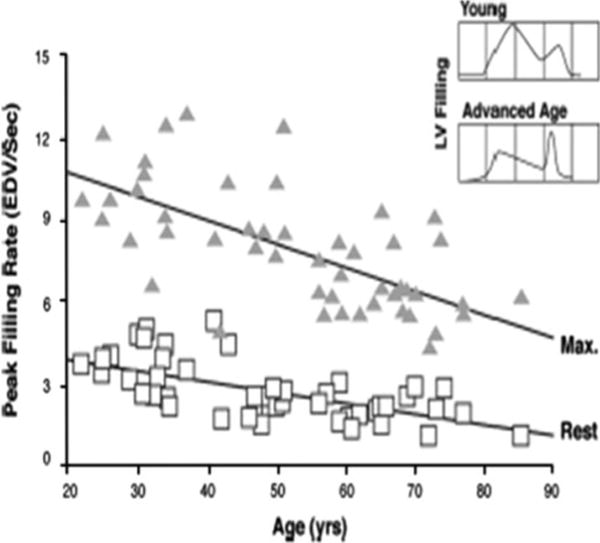
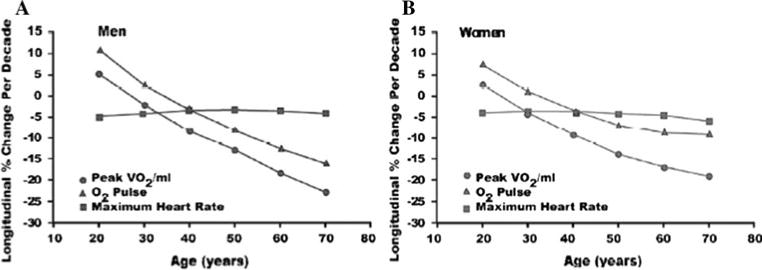
Important changes occur in the cardiovascular system with advancing age, even in apparently healthy individuals. Thickening and stiffening of the large arteries develop due to collagen and calcium deposition and loss of elastic fibers in the medial layer. These arterial changes cause systolic blood pressure to rise with age, while diastolic blood pressure generally declines after the sixth decade. In the left ventricle, modest concentric wall thickening occurs due to cellular hypertrophy, but cavity size does not change. Although left ventricular systolic function is preserved across the age span, early diastolic filling rate declines 30-50% between the third and ninth decades. Conversely, an age-associated increase in late diastolic filling due to atrial contraction preserves end-diastolic volume. Aerobic exercise capacity declines approximately 10% per decade in cross-sectional studies; in longitudinal studies, however, this decline is accelerated in the elderly. Reductions in peak heart rate and peripheral oxygen utilization but not stroke volume appear to mediate the age-associated decline in aerobic capacity. Deficits in both cardiac β-adrenergic receptor density and in the efficiency of postsynaptic β-adrenergic signaling contribute significantly to the reduced cardiovascular performance during exercise in older adults. Although these cardiovascular aging changes are considered "normative", they lower the threshold for the development of cardiovascular disease, which affects the majority of older adults.
Figures
References
-
- U. S. Census Bureau. National population projections. link: http://www.census.gov/population/www/projections/summarytables.html.
-
- Gerstenblith G, Frederiksen J, Yin FC, et al. Echocardiographic assessment of a normal adult aging population. Circulation. 1977;56:273–278. - PubMed
-
- Nagai Y, Metter EJ, Earley CJ, et al. Increased carotid artery intimal-medial thickness in asymptomatic older subjects with exercise-induced myocardial ischemia. Circulation. 1998;98:1504–1509. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
