

Imaging-based treatment selection for intravenous and intra-arterial stroke therapies: a comprehensive review
- PMID: 21809968
- PMCID: PMC3162247
- DOI: 10.1586/erc.11.56
Imaging-based treatment selection for intravenous and intra-arterial stroke therapies: a comprehensive review
Abstract
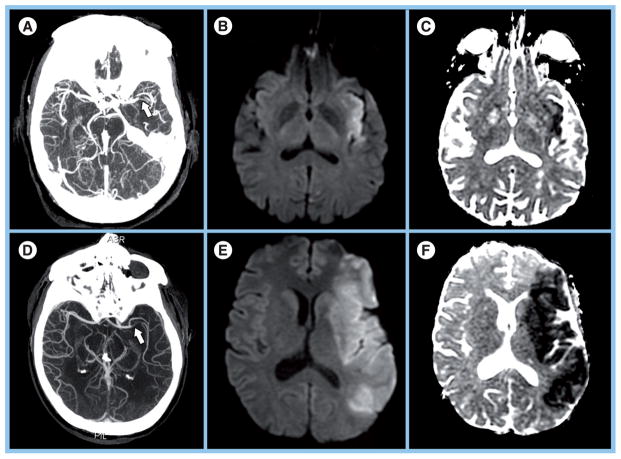
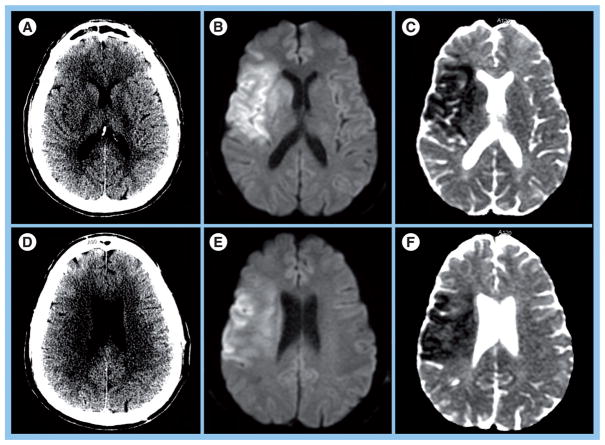
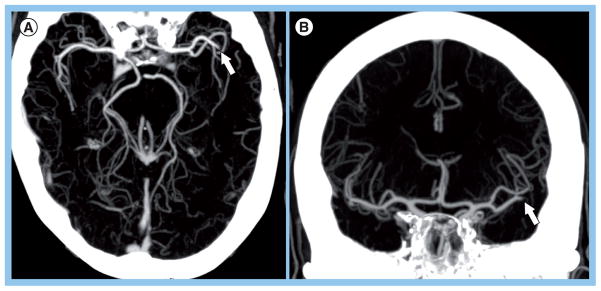
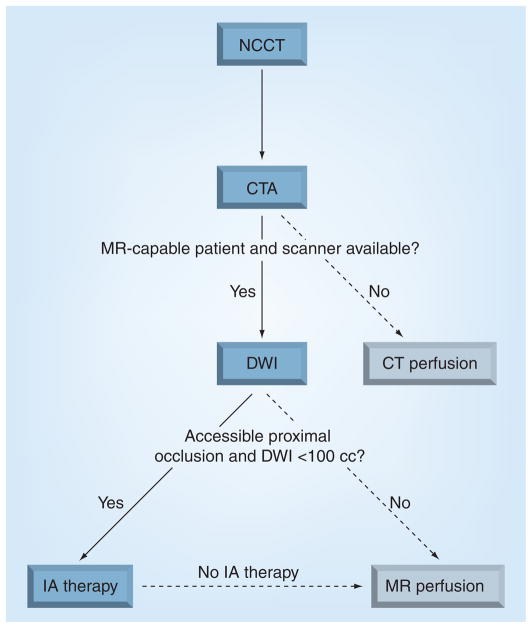
Reperfusion therapy is the only approved treatment for acute ischemic stroke. The current approach to patient selection is primarily based on the time from stroke symptom onset. However, this algorithm sharply restricts the eligible patient population, and neglects large variations in collateral circulation that ultimately determine the therapeutic time window in individual patients. Time alone is unlikely to remain the dominant parameter. Alternative approaches to patient selection involve advanced neuroimaging methods including MRI diffusion-weighted imaging, magnetic resonance and computed tomography perfusion imaging and noninvasive angiography that provide potentially valuable information regarding the state of the brain parenchyma and the neurovasculature. These techniques have now been used extensively, and there is emerging evidence on how specific imaging data may result in improved clinical outcomes. This article will review the major studies that have investigated the role of imaging in patient selection for both intravenous and intra-arterial therapies.
Figures
Similar articles
-
Trial design and reporting standards for intra-arterial cerebral thrombolysis for acute ischemic stroke.Stroke. 2003 Aug;34(8):e109-37. doi: 10.1161/01.STR.0000082721.62796.09. Epub 2003 Jul 17. Stroke. 2003. PMID: 12869717
-
Extending reperfusion therapy for acute ischemic stroke: emerging pharmacological, mechanical, and imaging strategies.Stroke. 2005 Oct;36(10):2311-20. doi: 10.1161/01.STR.0000182100.65262.46. Epub 2005 Sep 22. Stroke. 2005. PMID: 16179577 Review.
-
Advanced neuroimaging in acute ischemic stroke: extending the time window for treatment.Neurosurg Focus. 2011 Jun;30(6):E5. doi: 10.3171/2011.3.FOCUS1146. Neurosurg Focus. 2011. PMID: 21631229 Review.
-
Reperfusion therapy in acute ischemic stroke: dawn of a new era?BMC Neurol. 2018 Jan 16;18(1):8. doi: 10.1186/s12883-017-1007-y. BMC Neurol. 2018. PMID: 29338750 Free PMC article. Review.
-
Extension of therapeutic window in ischemic stroke by selective mismatch imaging.Int J Stroke. 2019 Jun;14(4):351-358. doi: 10.1177/1747493019840936. Epub 2019 Apr 1. Int J Stroke. 2019. PMID: 30935350 Review.
Cited by
-
Baseline collateral status and infarct topography in post-ischaemic perilesional hyperperfusion: An arterial spin labelling study.J Cereb Blood Flow Metab. 2017 Mar;37(3):1148-1162. doi: 10.1177/0271678X16653133. Epub 2016 Jul 21. J Cereb Blood Flow Metab. 2017. PMID: 27256323 Free PMC article.
-
MRI profile and response to endovascular reperfusion after stroke (DEFUSE 2): a prospective cohort study.Lancet Neurol. 2012 Oct;11(10):860-7. doi: 10.1016/S1474-4422(12)70203-X. Epub 2012 Sep 4. Lancet Neurol. 2012. PMID: 22954705 Free PMC article.
-
Systematic review with network meta-analysis: Diagnostic values of ultrasonography, computed tomography, and magnetic resonance imaging in patients with ischemic stroke.Medicine (Baltimore). 2019 Jul;98(30):e16360. doi: 10.1097/MD.0000000000016360. Medicine (Baltimore). 2019. PMID: 31348236 Free PMC article.
-
Acute stroke imaging: what is sufficient for triage to endovascular therapies?AJNR Am J Neuroradiol. 2012 May;33(5):790-2. doi: 10.3174/ajnr.A3098. Epub 2012 Mar 29. AJNR Am J Neuroradiol. 2012. PMID: 22460336 Free PMC article. No abstract available.
-
Multimodal CT imaging characteristics may predict post-reperfusion infarct volume in wake-up stroke patients.Quant Imaging Med Surg. 2023 Feb 1;13(2):878-888. doi: 10.21037/qims-22-614. Epub 2023 Jan 3. Quant Imaging Med Surg. 2023. PMID: 36819283 Free PMC article.
References
-
- Lloyd-Jones D, Adams R, Carnethon M, et al. Heart disease and stroke statistics – 2009 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2009;119(3):e21–e181. - PubMed
-
- Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. N Engl J Med. 1995;333(24):1581–1587. - PubMed
-
- Hacke W, Kaste M, Bluhmki E, et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med. 2008;359(13):1317–1329. - PubMed
Websites
-
- US National Institutes of Health. http://ClinicalTrials.gov.
-
- Internet Stroke Center, Washington University School of Medicine. Stroke Trials Registry. www.strokecenter.org/trials.
-
- BioMed Central. Current Controlled Trials. www.controlled-trials.com.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical