

Embryonal central nervous system neoplasms arising in infants and young children: a pediatric brain tumor consortium study
- PMID: 21809989
- PMCID: PMC3752842
- DOI: 10.5858/2010-0515-OAR1
Embryonal central nervous system neoplasms arising in infants and young children: a pediatric brain tumor consortium study
Abstract
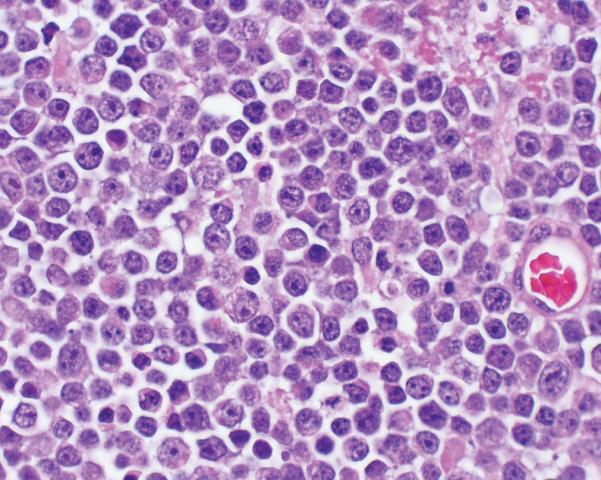
Context: Medulloblastomas (MBs) and atypical teratoid/rhabdoid tumors (AT/RTs) arising in infants and children can be difficult to distinguish; however, histologic characterization is prognostically important.
Objective: To determine histologic and phenotypic markers associated with utility with progression-free survival (PFS) and overall survival (OS) in children younger than 3 years with MBs and AT/RTs.
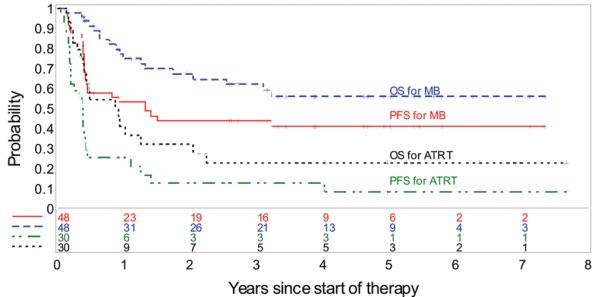
Design: We undertook a histologic and immunophenotypic study of MBs and AT/RTs arising in infants and children younger than 3 years treated in a Pediatric Brain Tumor Consortium study. The 41 girls and 55 boys ranged in age from 2 to 36 months at enrollment. These infants and children exhibited 51 MBs, 26 AT/RTs, and 24 other tumors (not further studied). Median follow-up of the patients was 17.2 months from diagnosis (range: 1.4-93 months).
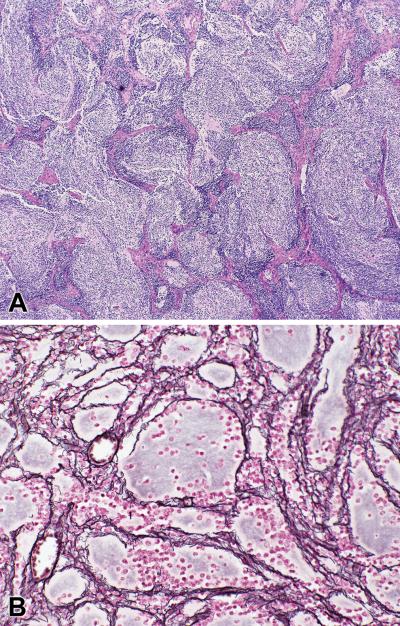
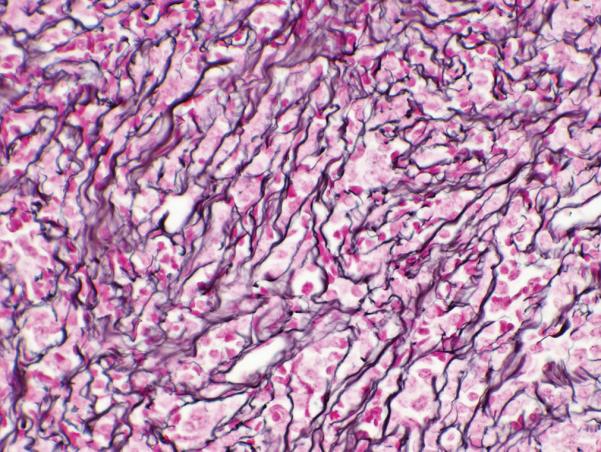
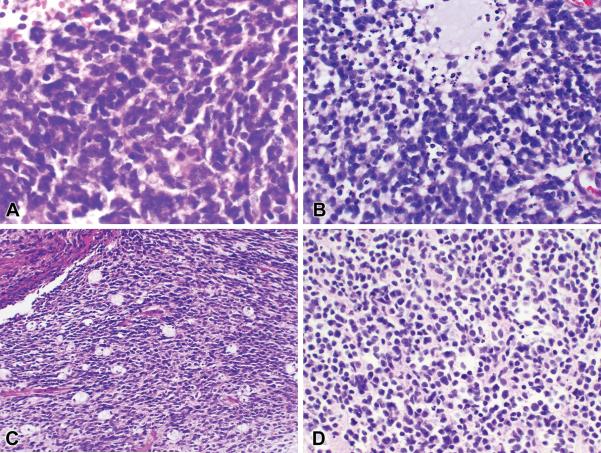
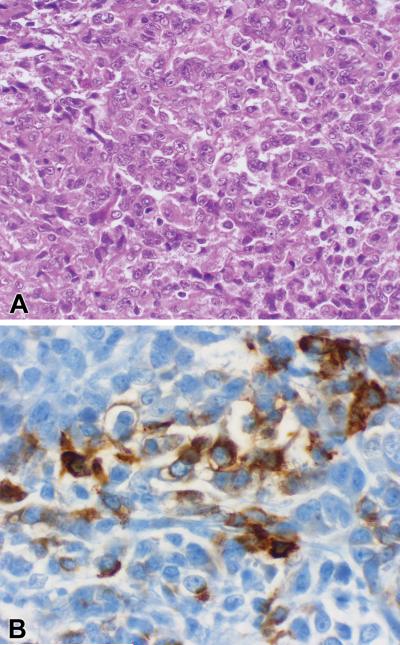
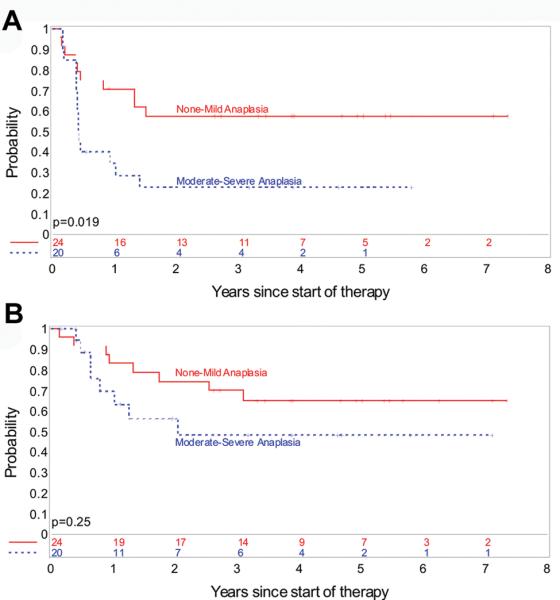
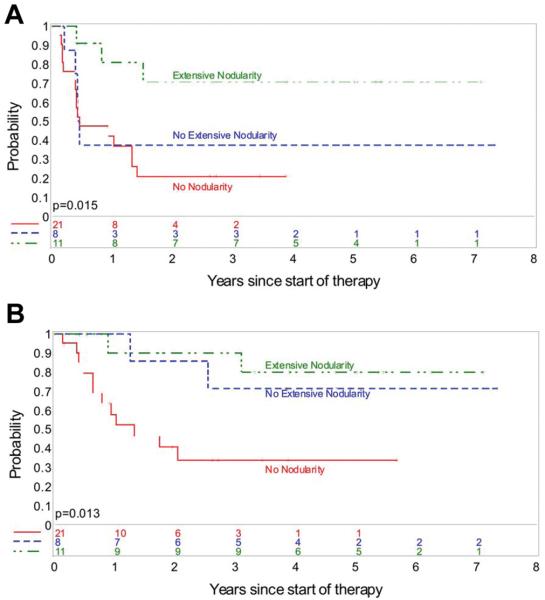
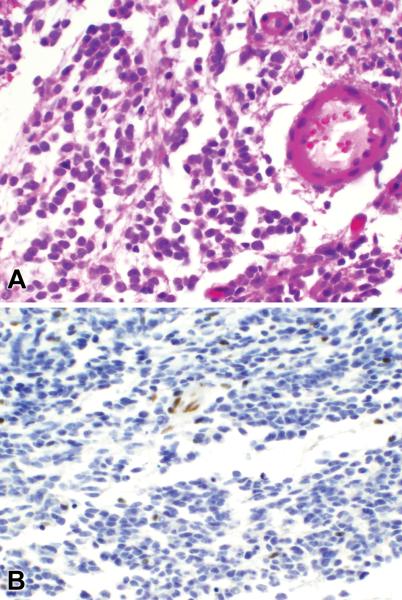
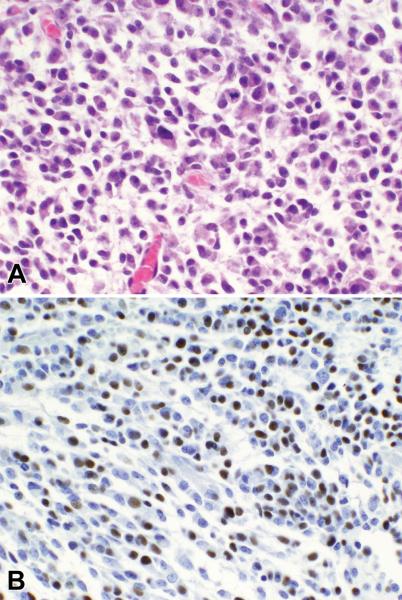
Results: Infants and children with AT/RT exhibited a statistically significant shorter PFS and OS when compared to infants and children with MBs (both P < .001). A lack of nuclear BAF47 immunohistochemical reactivity proved reliable in identifying AT/RTs. Among MBs, our data suggest an association of nodularity and prolonged PFS and OS, which must be independently confirmed. Anaplasia correlated with OTX2 reactivity and both OTX2 and moderate to severe anaplasia correlated with PFS but not with OS.
Conclusion: Distinguishing AT/RT from MBs is clinically important. For expert neuropathologists, the diagnoses of AT/RT and MB can be reliably made from hematoxylin-eosin stains in the vast majority of cases. However certain rare small cell variants of AT/RT can be confused with MB. We also found that immunohistochemical reactivity for BAF47 is clinically useful in distinguishing MBs from AT/RTs and for identifying certain small cell AT/RTs. Among MBs, nodularity may be an important prognostic factor for improved PFS and OS in infants and children.
Trial registration: ClinicalTrials.gov NCT00042367.
Figures
References
-
- CBTRUS . Supplement Report: Primary Brain Tumors in the United States, 2004. Central Brain Tumor Registry of the United States; Hinsdale, IL: 2008.
-
- Kleihues P, Burger P, Scheithauer BW, editors. Histological Typing of Tumours of the Central Nervous System. 2nd ed Springer-Verlag; Berlin: 1993.
-
- Lamont JM, McManamy CS, Pearson AD, Clifford SC, Ellison DW. Combined histopathological and molecular cytogenetic stratification of medulloblastoma patients. Clin Cancer Res. 2004;10(16):5482–5493. - PubMed
-
- Helseth E, Due-Tonnessen B, Wesenberg F, Lote K, Lundar T. Posterior fossa medulloblastoma in children and young adults (0–19 years): survival and performance. Childs Nerv Syst. 1999;15(9):451–455. discussion 456. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous