

HDL cholesterol and bone mineral density: is there a genetic link?
- PMID: 21810493
- PMCID: PMC3236254
- DOI: 10.1016/j.bone.2011.07.002
HDL cholesterol and bone mineral density: is there a genetic link?
Abstract
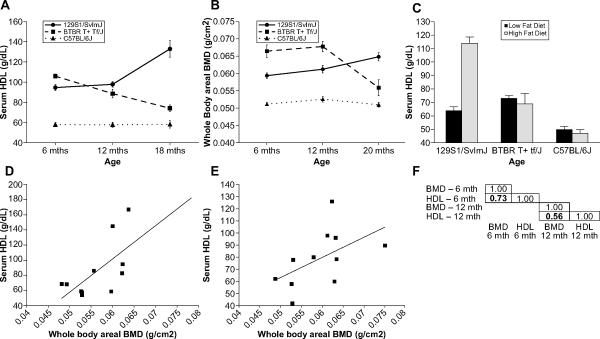
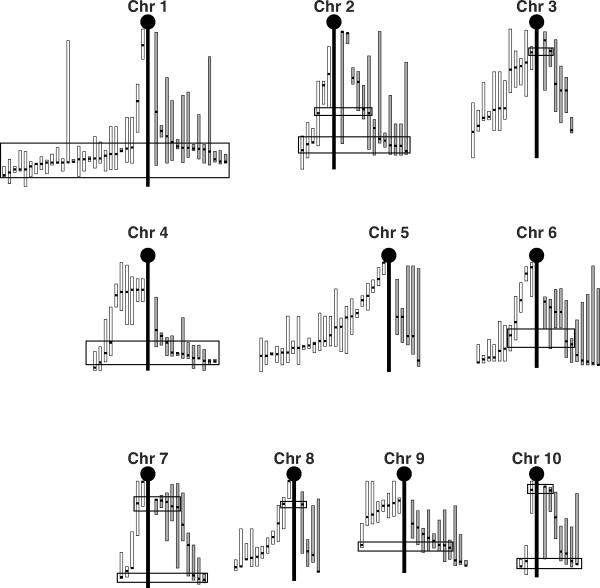
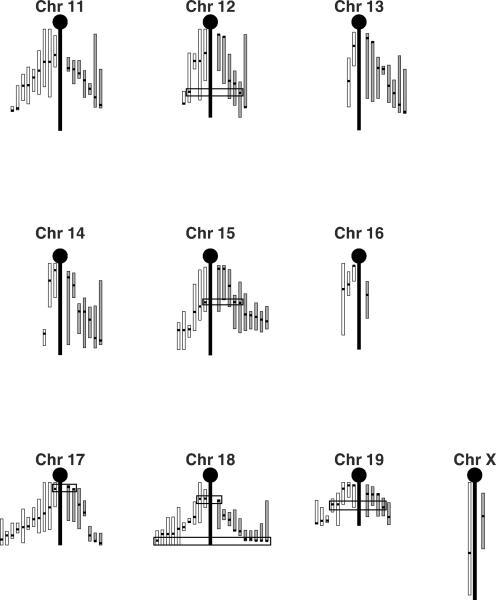
Overwhelming evidence has linked cardiovascular disease and osteoporosis, but the shared root cause of these two diseases of the elderly remains unknown. Low levels of high density lipoprotein cholesterol (HDL) and bone mineral density (BMD) are risk factors for cardiovascular disease and osteoporosis respectively. A number of correlation studies have attempted to determine if there is a relationship between serum HDL and BMD but these studies are confounded by a number of variables including age, diet, genetic background, gender and hormonal status. Collectively, these data suggest that there is a relationship between these two phenotypes, but that the nature of this relationship is context specific. Studies in mice plainly demonstrate that genetic loci for BMD and HDL co-map and transgenic mouse models have been used to show that a single gene can affect both serum HDL and BMD. Work completed to date has demonstrated that HDL can interact directly with both osteoblasts and osteoclasts, but no direct evidence links bone back to the regulation of HDL levels. Understanding the genetic relationship between BMD and HDL has huge implications for understanding the clinical relationship between CVD and osteoporosis and for the development of safe treatment options for both diseases.
Copyright © 2011 Elsevier Inc. All rights reserved.
Figures
References
-
- Anderson JB, Barnett E, Nordin BE. The Relation between Osteoporosis and Aortic Calcification. Br J Radiol. 1964;37:910–2. - PubMed
-
- Heidenreich PA, Trogdon JG, Khavjou OA, Butler J, Dracup K, Ezekowitz MD, Finkelstein EA, Hong Y, Johnston SC, Khera A, Lloyd-Jones DM, Nelson SA, Nichol G, Orenstein D, Wilson PW, Woo YJ. Forecasting the Future of Cardiovascular Disease in the United States: A Policy Statement From the American Heart Association. Circulation. 2011 - PubMed
-
- Services USDoHaH . Bone Health and Osteoporosis: A Report of the Surgeon General. U.S. Department of Health and Human Services, Office of the Surgeon General; Rockville, MD: 2004. - PubMed
-
- Qi L, Shen H, Ordovas JM. Hearts and bones. Nutr Metab Cardiovasc Dis. 2003;13:165–74. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
