

Treatment outcomes and cost-effectiveness of shifting management of stable ART patients to nurses in South Africa: an observational cohort
- PMID: 21811402
- PMCID: PMC3139666
- DOI: 10.1371/journal.pmed.1001055
Treatment outcomes and cost-effectiveness of shifting management of stable ART patients to nurses in South Africa: an observational cohort
Abstract
Background: To address human resource and infrastructure shortages, resource-constrained countries are being encouraged to shift HIV care to lesser trained care providers and lower level health care facilities. This study evaluated the cost-effectiveness of down-referring stable antiretroviral therapy (ART) patients from a doctor-managed, hospital-based ART clinic to a nurse-managed primary health care facility in Johannesburg, South Africa.
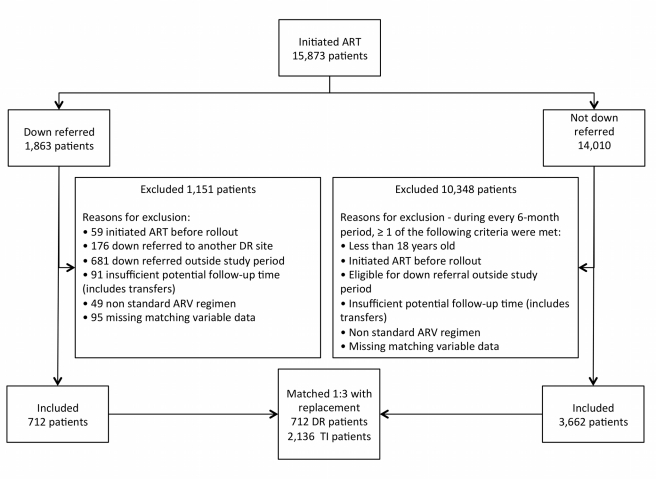
Methods and findings: Criteria for down-referral were stable ART (≥11 mo), undetectable viral load within the previous 10 mo, CD4>200 cells/mm(3), <5% weight loss over the last three visits, and no opportunistic infections. All patients down-referred from the treatment-initiation site to the down-referral site between 1 February 2008 and 1 January 2009 were compared to a matched sample of patients eligible for down-referral but not down-referred. Outcomes were assigned based on vital and health status 12 mo after down-referral eligibility and the average cost per outcome estimated from patient medical record data. The down-referral site (n = 712) experienced less death and loss to follow up than the treatment-initiation site (n = 2,136) (1.7% versus 6.2%, relative risk = 0.27, 95% CI 0.15-0.49). The average cost per patient-year for those in care and responding at 12 mo was US$492 for down-referred patients and US$551 for patients remaining at the treatment-initiation site (p<0.0001), a savings of 11%. Down-referral was the cost-effective strategy for eligible patients.
Conclusions: Twelve-month outcomes of stable ART patients who are down-referred to a primary health clinic are as good as, or better than, the outcomes of similar patients who are maintained at a hospital-based ART clinic. The cost of treatment with down-referral is lower across all outcomes and would save 11% for patients who remain in care and respond to treatment. These results suggest that this strategy would increase treatment capacity and conserve resources without compromising patient outcomes.
Conflict of interest statement
The authors have declared no competing interests. IS is the director and IJ an employee of Right to Care, an organization that provides technical assistance to the study sites.
Figures

Comment in
-
Simplified ART delivery models are needed for the next phase of scale up.PLoS Med. 2011 Jul;8(7):e1001060. doi: 10.1371/journal.pmed.1001060. Epub 2011 Jul 19. PLoS Med. 2011. PMID: 21811405 Free PMC article.
References
-
- World Health Organization. Task shifting: rational redistribution of tasks among health workforce teams: global recommendations and guidelines. Geneva: World Health Organization; 2008. Available: http://www.who.int/healthsystems/TTR-TaskShifting.pdf. Accessed 2 November 2010.
-
- Callaghan M, Ford N, Schneider H. A systematic review of task- shifting for HIV treatment and care in Africa. Hum Resour Health. 2010;8:8. doi: 10.1186/1478-4491-8-8. - DOI - PMC - PubMed
-
- Bedelu M, Ford N, Hilderbrand K, Reuter H. Implementing antiretroviral therapy in rural communities: the Lusikisiki model of decentralized HIV/AIDS care. J Infect Dis. 2007;196(Suppl):S464–S468. - PubMed
-
- Fatti G, Grimwood A, Bock P. Better antiretroviral therapy outcomes at primary healthcare facilities: an evaluation of three tiers of ART services in four South African provinces. PLoS ONE. 2010;5:e12888. doi: 10.1371/journal.pone.0012888. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
