

Septic shock due to candidemia: outcomes and predictors of shock development
- PMID: 21811532
- PMCID: PMC3140925
- DOI: 10.4021/jocmr536w
Septic shock due to candidemia: outcomes and predictors of shock development
Abstract
Background: The present report describes the outcomes of a cohort of patients with Candida induced septic shock.
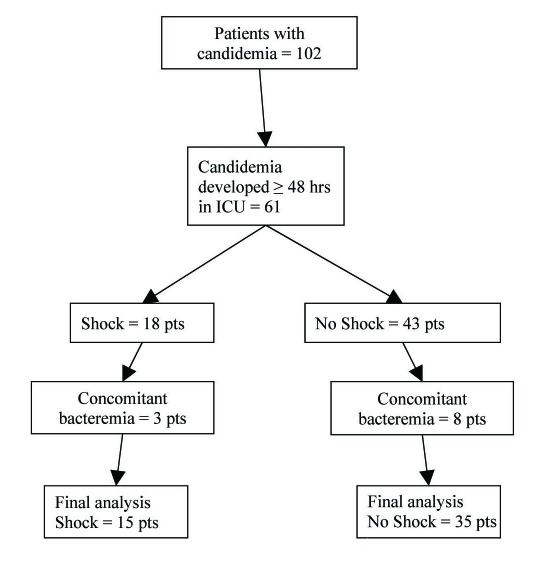
Methods: Retrospective analysis of individuals who had at least one positive blood culture for Candida species ≥ 48 h after ICU admission. Data from patients that developed septic shock within 48 hr of the positive blood culture were compared to non-shock candidemic patients. Patients with a concomitant bacteremia and/or endocarditis were excluded.
Results: Fifteen patients with Candida induced septic shock were studied and compared to 35 candidemic patients without shock. Overall mortality was 76% (87 % among those who had shock). A high proportion of non-albicans Candida species causing fungemia (74%) was observed. All patients with shock were receiving antibiotics but not antifungal treatment at the time of shock development, eight were on parenteral nutrition, six on steroids and nine had a cancer history. High dose fluconazole was the most common initial treatment provided. Four patients died before receiving any antifungal treatment. Time in ICU before the development of candidemia was identified as a predictor of shock development (higher chance if fungemia developed < 7 days after ICU admission).
Conclusions: Septic shock due to invasive candidiasis is a near fatal condition. No conventional risk factors were identified to predict shock development other than time (shorter) spent in ICU before the development of candidemia. We encourage clinicians to consider the initiation of appropriate empiric antifungal treatment in high-risk patients who develop septic shock while on antimicrobial treatment.
Keywords: Septic shock; Candidemia; Outcome; Predictor.
Figures
References
-
- Edmond MB, Wallace SE, McClish DK, Pfaller MA, Jones RN, Wenzel RP. Nosocomial bloodstream infections in United States hospitals: a three-year analysis. Clin Infect Dis. 1999;29(2):239–244. - PubMed
-
- Pfaller MA, Diekema DJ, Jones RN, Sader HS, Fluit AC, Hollis RJ, Messer SA. International surveillance of bloodstream infections due to Candida species: frequency of occurrence and in vitro susceptibilities to fluconazole, ravuconazole, and voriconazole of isolates collected from 1997 through 1999 in the SENTRY antimicrobial surveillance program. J Clin Microbiol. 2001;39(9):3254–3259. - PMC - PubMed
-
- Marchetti O, Bille J, Fluckiger U, Eggimann P, Ruef C, Garbino J, Calandra T. et al. Epidemiology of candidemia in Swiss tertiary care hospitals: secular trends, 1991-2000. Clin Infect Dis. 2004;38(3):311–320. - PubMed
-
- Nguyen MH, Peacock JE Jr., Morris AJ, Tanner DC, Nguyen ML, Snydman DR, Wagener MM. et al. The changing face of candidemia: emergence of non-Candida albicans species and antifungal resistance. Am J Med. 1996;100(6):617–623. - PubMed
-
- Eggimann P, Garbino J, Pittet D. Epidemiology of Candida species infections in critically ill non-immunosuppressed patients. Lancet Infect Dis. 2003;3(11):685–702. - PubMed
LinkOut - more resources
Full Text Sources