

Revisiting traditional risk factors for rejection and graft loss after kidney transplantation
- PMID: 21812918
- PMCID: PMC3184338
- DOI: 10.1111/j.1600-6143.2011.03640.x
Revisiting traditional risk factors for rejection and graft loss after kidney transplantation
Abstract
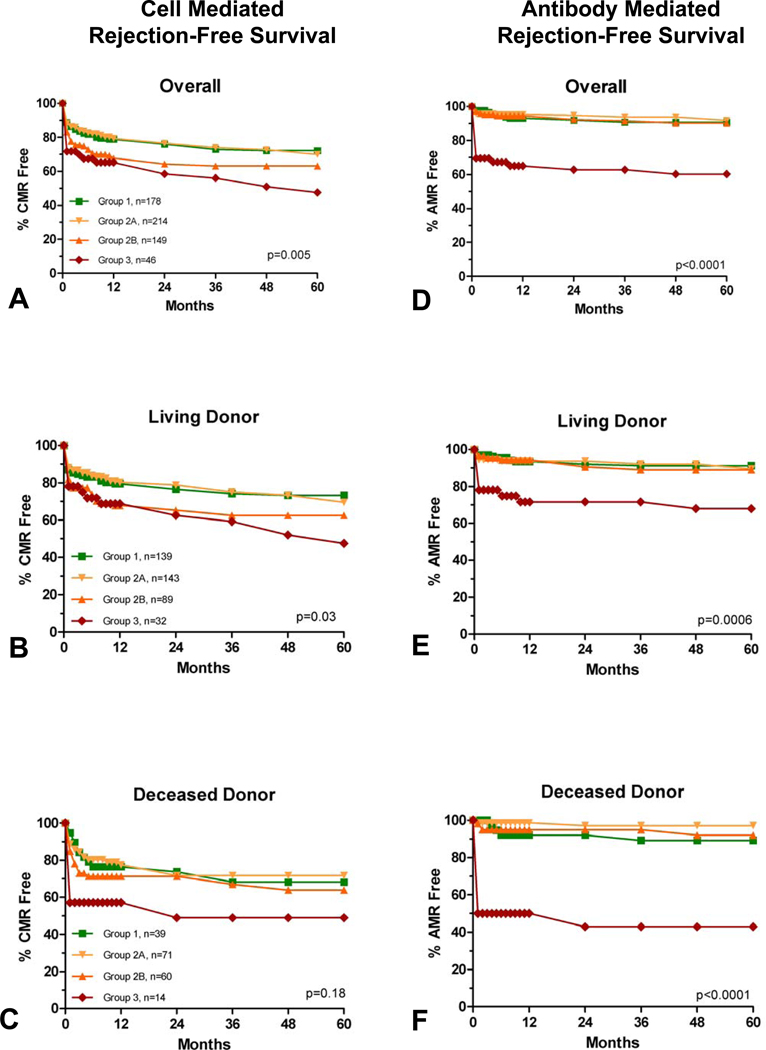
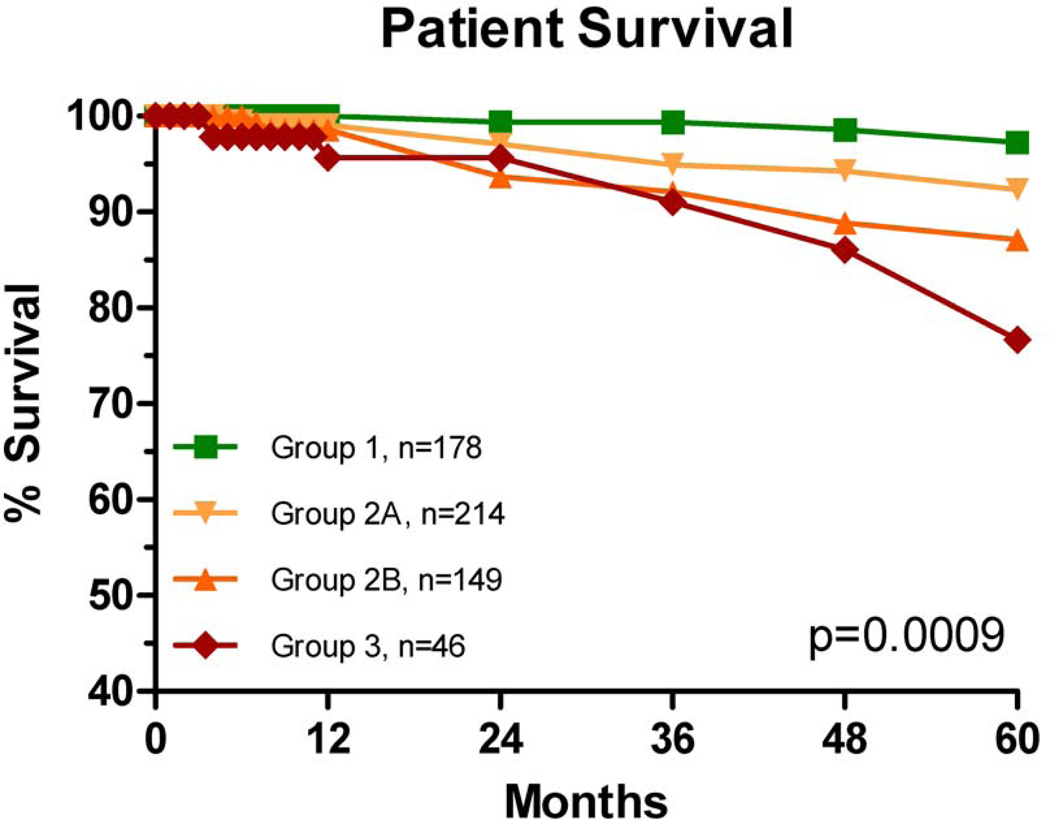
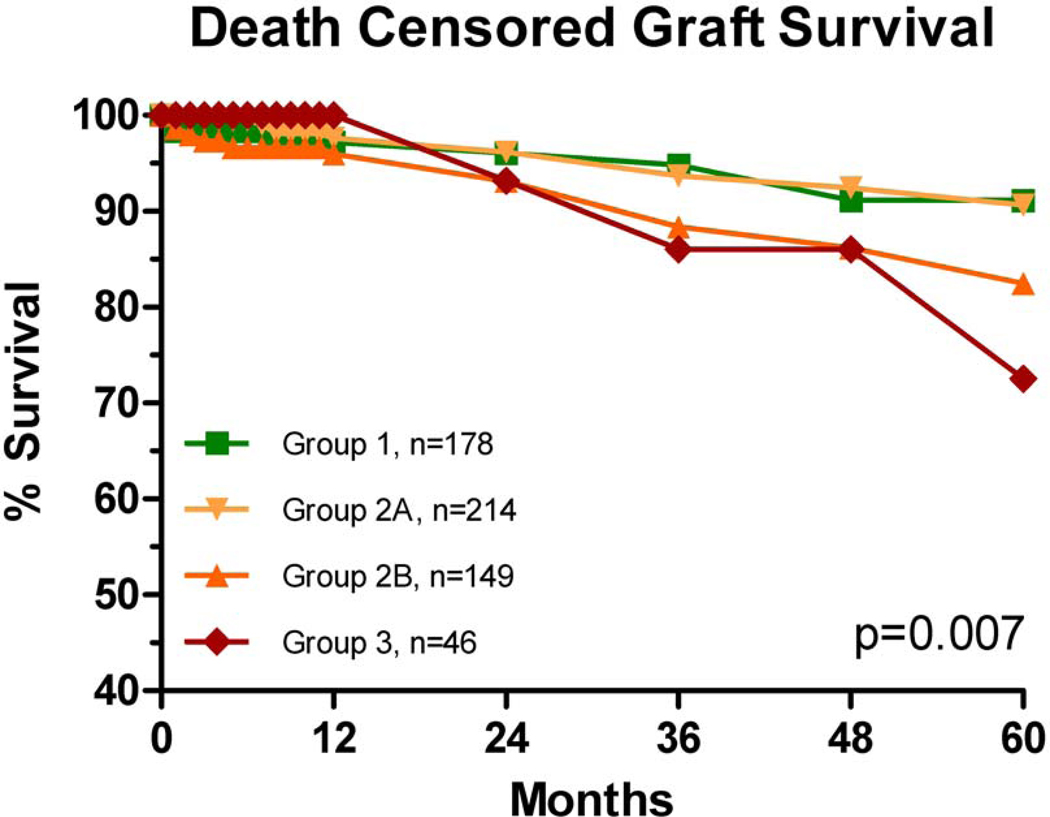
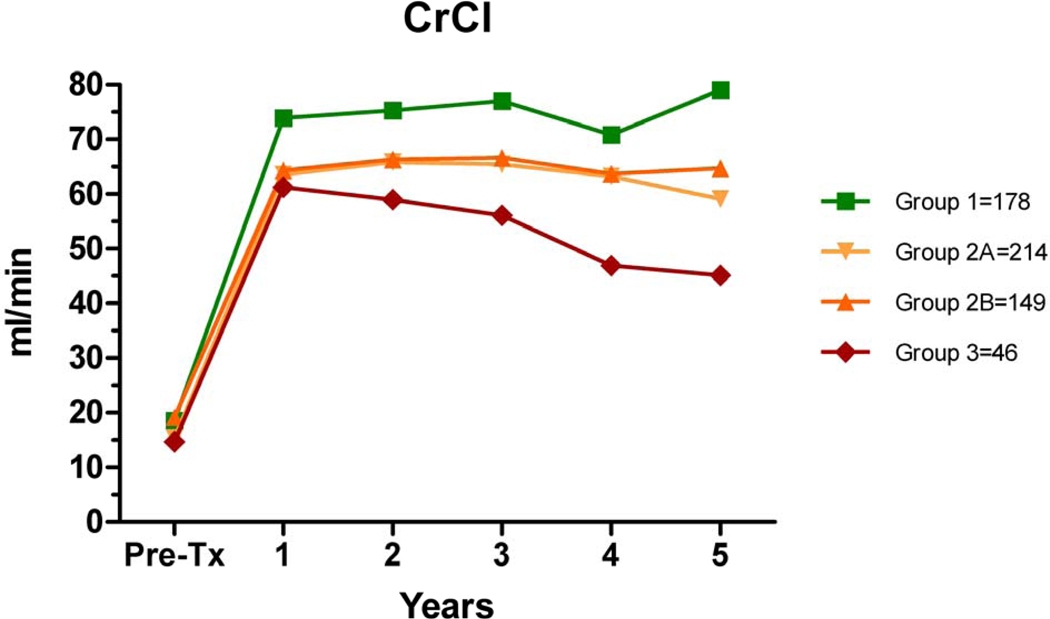
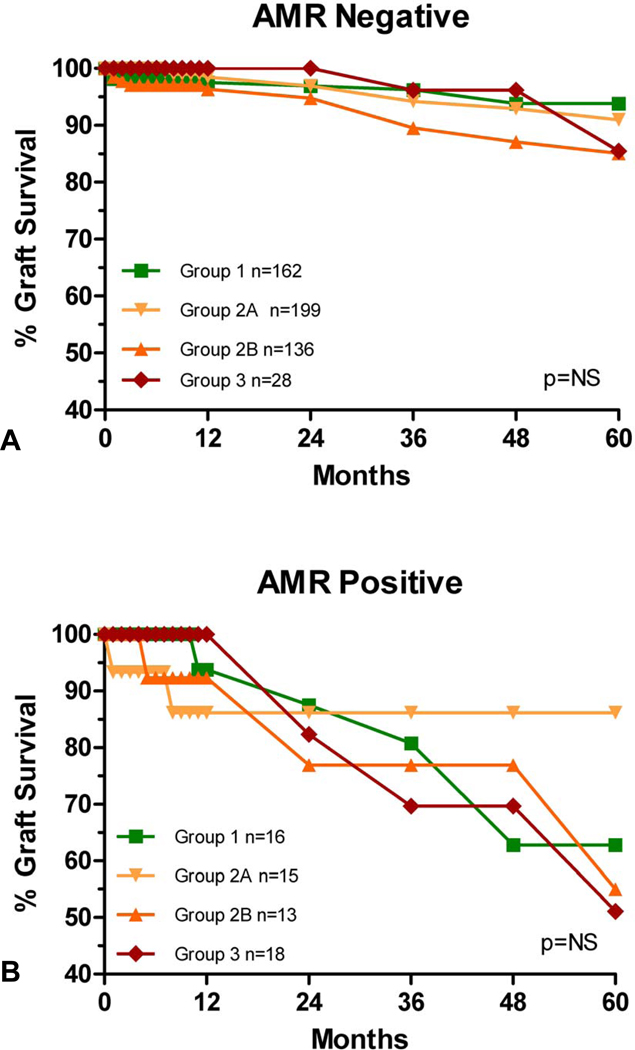
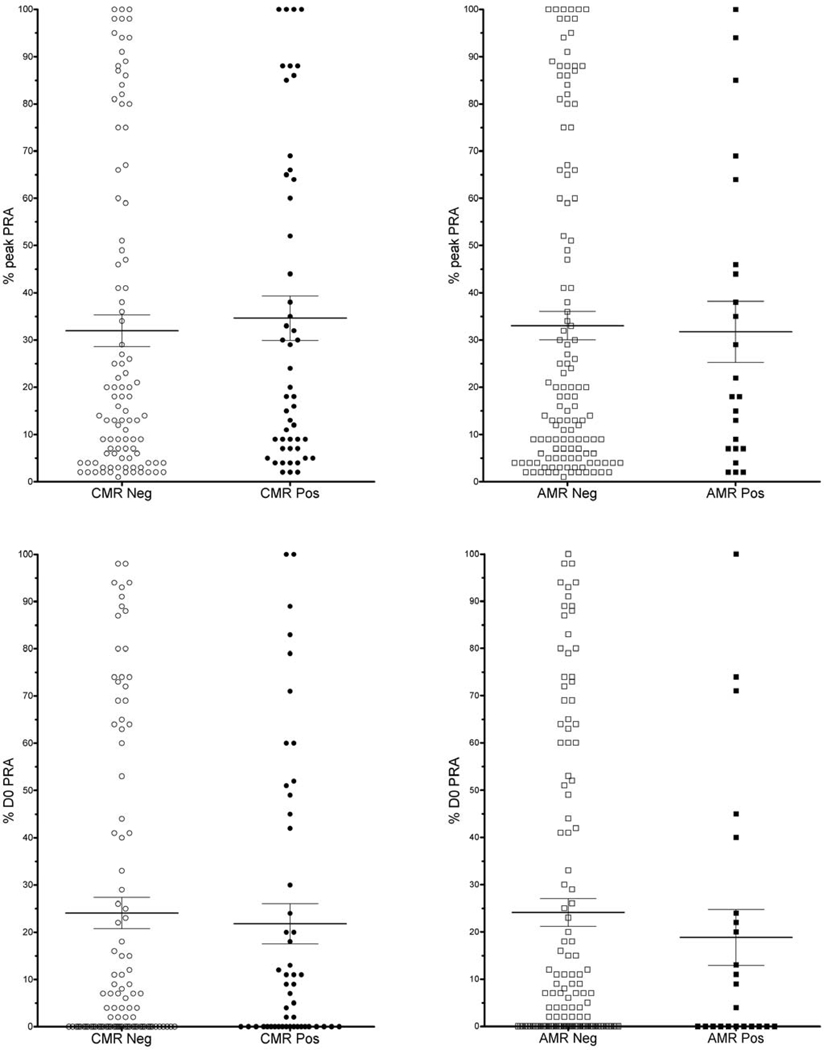
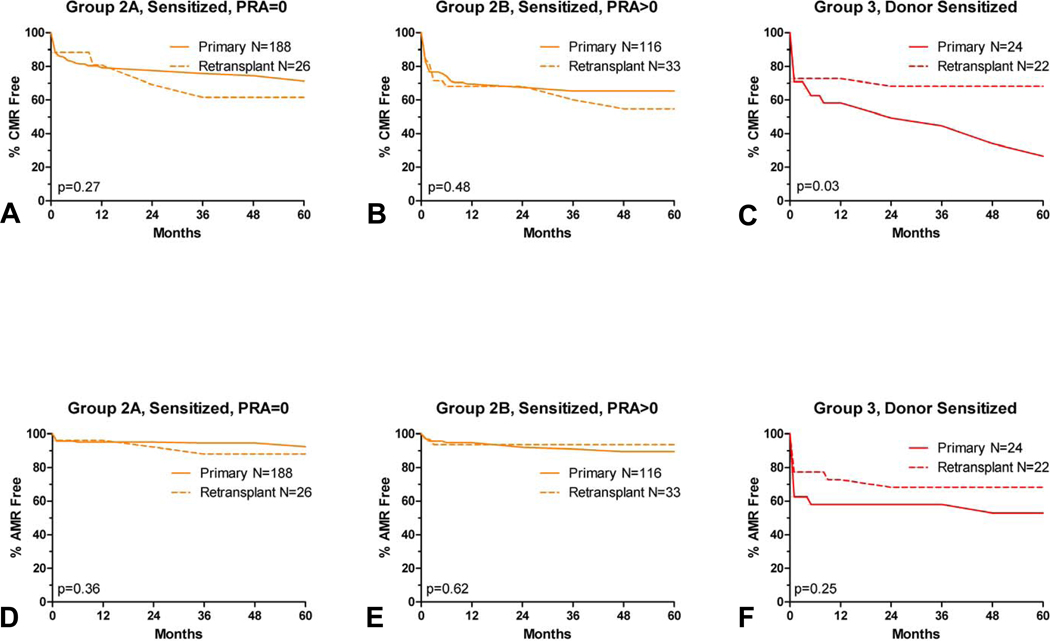
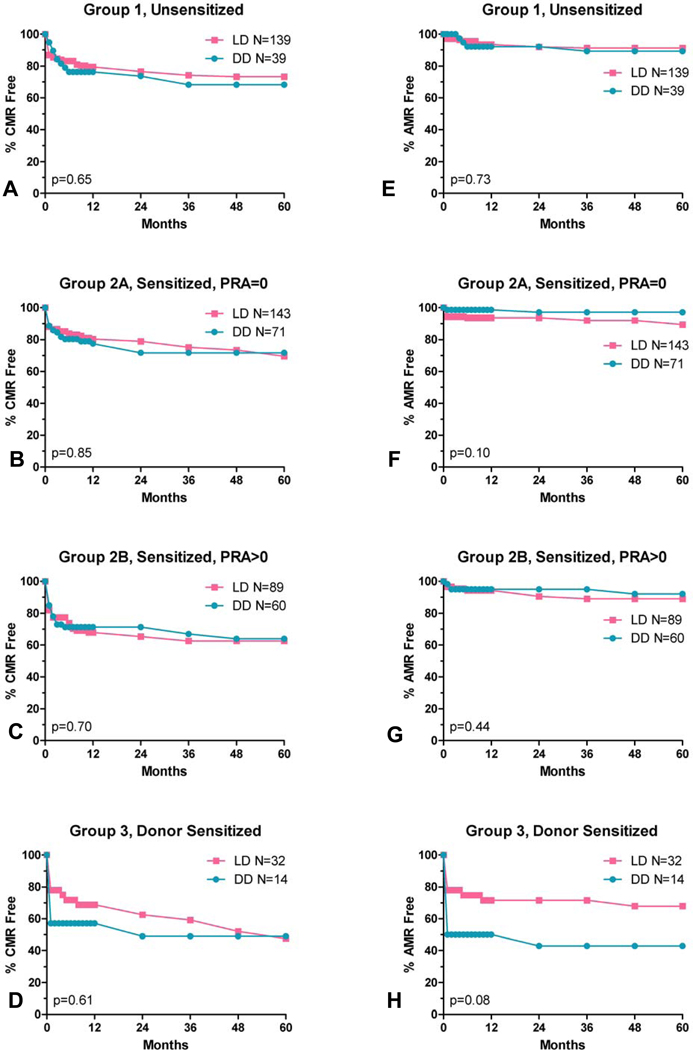
Single-antigen bead (SAB) testing permits reassessment of immunologic risk for kidney transplantation. Traditionally, high panel reactive antibody (PRA), retransplant and deceased donor (DD) grafts have been associated with increased risk. We hypothesized that this risk was likely mediated by (unrecognized) donor-specific antibody (DSA). We grouped 587 kidney transplants using clinical history and single-antigen bead (SAB) testing of day of transplant serum as (1) unsensitized; PRA = 0 (n = 178), (2) third-party sensitized; no DSA (n = 363) or (3) donor sensitized; with DSA (n = 46), and studied rejection rates, death-censored graft survival (DCGS) and risk factors for rejection. Antibody-mediated rejection (AMR) rates were increased with DSA (p < 0.0001), but not with panel reactive antibody (PRA) in the absence of DSA. Cell-mediated rejection (CMR) rates were increased with DSA (p < 0.005); with a trend to increased rates when PRA>0 in the absence of DSA (p = 0.08). Multivariate analyses showed risk factors for AMR were DSA, worse HLA matching, and female gender; for CMR: DSA, PRA>0 and worse HLA matching. AMR and CMR were associated with decreased DCGS. The presence of DSA is an important predictor of rejection risk, in contrast to traditional risk factors. Further development of immunosuppressive protocols will be facilitated by stratification of rejection risk by donor sensitization.
©2011 The Authors Journal compilation©2011 The American Society of Transplantation and the American Society of Transplant Surgeons.
Conflict of interest statement
The authors of this manuscript have no conflicts of interest to disclose as described by the American Journal of Transplantation.
Figures
References
-
- Bryan CF, Baier KA, Nelson PW, Luger AM, Martinez J, Pierce GE, et al. Long-term graft survival is improved in cadaveric renal retransplantation by flow cytometric crossmatching. Transplantation. 1998 Dec 27;66(12):1827–1832. - PubMed
-
- Kerman RH, Orosz CG, Lorber MI. Clinical relevance of anti-HLA antibodies pre and post transplant. Am J Med Sci. 1997 May;313(5):275–278. - PubMed
-
- Gebel HM, Bray RA. Sensitization and sensitivity: defining the unsensitized patient. Transplantation. 2000 Apr 15;69(7):1370–1374. - PubMed
-
- Zeevi A, Girnita A, Duquesnoy R. HLA antibody analysis: sensitivity, specificity, and clinical significance in solid organ transplantation. Immunol Res. 2006;36(1–3):255–264. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
