

Multicentre validation of the bedside paediatric early warning system score: a severity of illness score to detect evolving critical illness in hospitalised children
- PMID: 21812993
- PMCID: PMC3387627
- DOI: 10.1186/cc10337
Multicentre validation of the bedside paediatric early warning system score: a severity of illness score to detect evolving critical illness in hospitalised children
Abstract
Introduction: The timely provision of critical care to hospitalised patients at risk for cardiopulmonary arrest is contingent upon identification and referral by frontline providers. Current approaches require improvement. In a single-centre study, we developed the Bedside Paediatric Early Warning System (Bedside PEWS) score to identify patients at risk. The objective of this study was to validate the Bedside PEWS score in a large patient population at multiple hospitals.
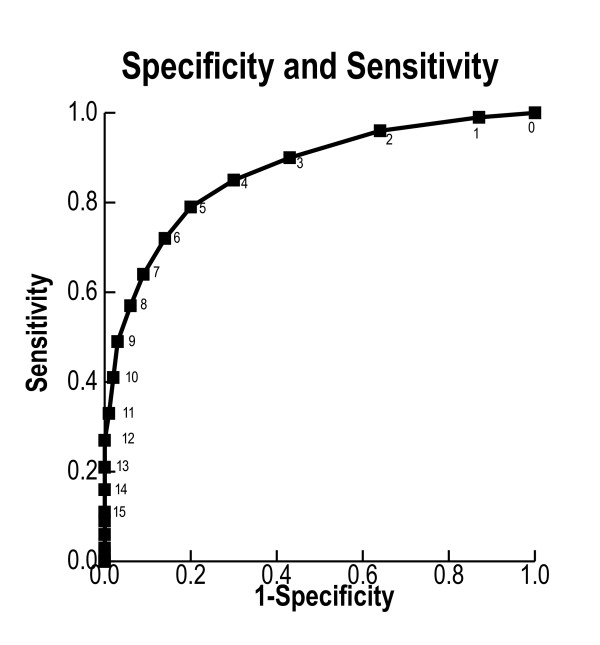
Methods: We performed an international, multicentre, case-control study of children admitted to hospital inpatient units with no limitations on care. Case patients had experienced a clinical deterioration event involving either an immediate call to a resuscitation team or urgent admission to a paediatric intensive care unit. Control patients had no events. The scores ranged from 0 to 26 and were assessed in the 24 hours prior to the clinical deterioration event. Score performance was assessed using the area under the receiver operating characteristic (AUCROC) curve by comparison with the retrospective rating of nurses and the temporal progression of scores in case patients.
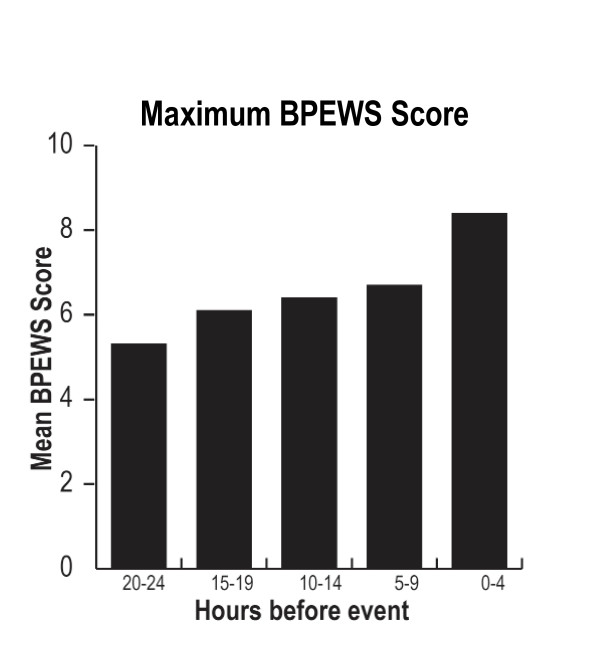
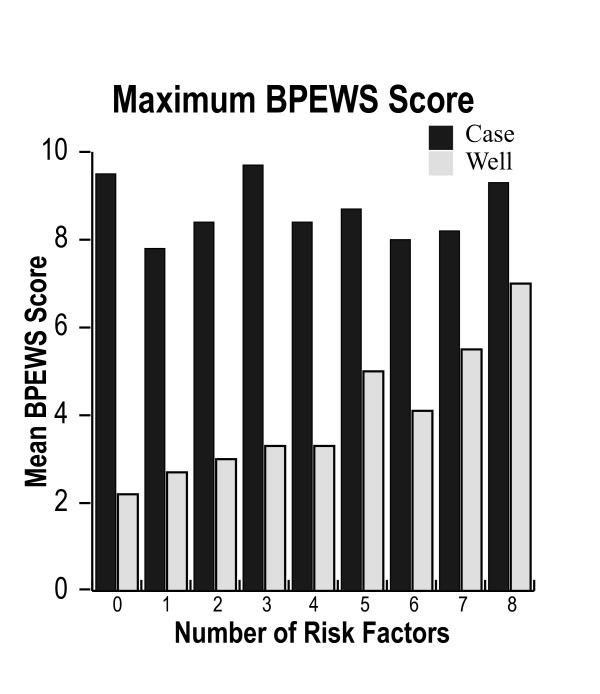
Results: A total of 2,074 patients were evaluated at 4 participating hospitals. The median (interquartile range) maximum Bedside PEWS scores for the 12 hours ending 1 hour before the clinical deterioration event were 8 (5 to 12) in case patients and 2 (1 to 4) in control patients (P < 0.0001). The AUCROC curve (95% confidence interval) was 0.87 (0.85 to 0.89). In case patients, mean scores were 5.3 at 20 to 24 hours and 8.4 at 0 to 4 hours before the event (P < 0.0001). The AUCROC curve (95% CI) of the retrospective nurse ratings was 0.83 (0.81 to 0.86). This was significantly lower than that of the Bedside PEWS score (P < 0.0001).
Conclusions: The Bedside PEWS score identified children at risk for cardiopulmonary arrest. Scores were elevated and continued to increase in the 24 hours before the clinical deterioration event. Prospective clinical evaluation is needed to determine whether this score will improve the quality of care and patient outcomes.
Figures
References
-
- Hillman K, Chen J, Cretikos M, Bellomo R, Brown D, Doig G, Finfer S, Flabouris A. Introduction of the medical emergency team (MET) system: a cluster-randomised controlled trial. Lancet. 2005;365:2091–2097. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
