

New hepatitis C therapies in clinical development
- PMID: 21813371
- PMCID: PMC3352002
- DOI: 10.1186/2047-783x-16-7-303
New hepatitis C therapies in clinical development
Abstract
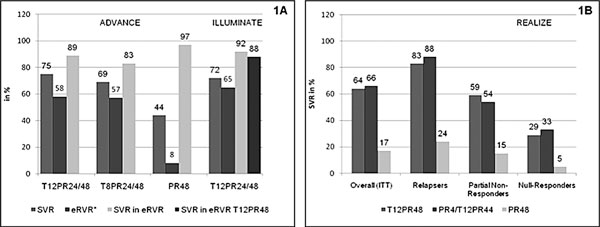
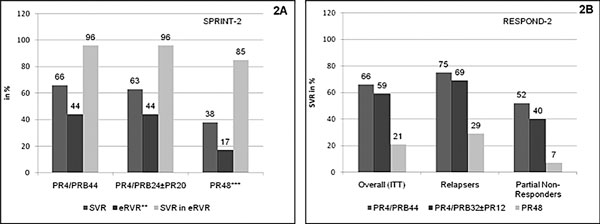
With the current standard of care for the treatment of chronic hepatitis C, a combination of pegylated interferon alfa and ribavirin, sustained virologic response rates can be achieved in approximately 50% of patients only. - Improved understanding of the viral life cycle has led to the identification of numerous potential targets for novel, direct-acting antiviral compounds. Inhibitors of the NS3/4A protease are currently the most advanced in clinical development. Recently completed phase 3 studies of the two protease inhibitors telaprevir and boceprevir, each given in combination with standard of care, yielded sustained virologic response rates in the range of 66-75% in treatment-naive patients and 59-66% in treatment-experienced patients with HCV genotype 1 infection. Studies of second-generation protease inhibitors, with the potential advantage of improved potency, drug metabolism and pharmacokinetics profile, are already underway. - Inhibitors of the HCV NS5A protein and NS5B polymerase are potentially active across different HCV genotypes and have shown promising antiviral efficacy in early clinical studies. Other emerging mechanisms include silymarin components and inhibitors of cell proteins required for HCV replication. - While improved formulations of current HCV therapies are also being developed, future hopes lie on the combination of direct-acting antivirals with the eventual possibility of interferon-free treatment regimens.
Figures
References
-
- Hepatitis C. World Health Organization. http://www.who.int/csr/disease/hepatitis/whocdscsrlyo2003/en/index4.html accessed on 01.12.2010.
-
- Hadziyannis SJ, Sette H, Morgan TR. et al.Peginterferon-alpha2a and ribavirin combination therapy in chronic hepatitis C: a randomized study of treatment duration and ribavirin dose. Ann Intern Med. 2004;140:346–355. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
